
Introduction
Around 1.1 billion people worldwide suffer from visual impairment, and that number is expected to rise significantly in the coming decades according to global health data. Artificial intelligence has emerged as a transformative force in ophthalmology, reshaping how clinicians detect, diagnose, and treat eye diseases at every stage. The field is uniquely suited for AI integration because it generates massive volumes of high-resolution digital images through modalities like fundus photography and optical coherence tomography. A recent survey found that 78% of ophthalmologists identified AI as the most transformative trend shaping their specialty in 2025. From autonomous diabetic retinopathy screening to AI-guided cataract surgery planning, these tools are expanding access to eye care in underserved communities worldwide. The convergence of deep learning, computer vision, and clinical imaging data is creating a new era in ophthalmic medicine that promises earlier detection and better outcomes for millions of patients. The global AI in ophthalmology market was valued at approximately $314.64 million in 2025, and projections indicate explosive growth at a compound annual growth rate of 36.8% through 2035.
Key Questions
What is the role of AI in ophthalmology?
AI in ophthalmology uses deep learning algorithms to analyze retinal images, OCT scans, and clinical data for automated detection, diagnosis, and monitoring of eye diseases including diabetic retinopathy, glaucoma, and macular degeneration.
Which AI system was first approved for eye disease detection?
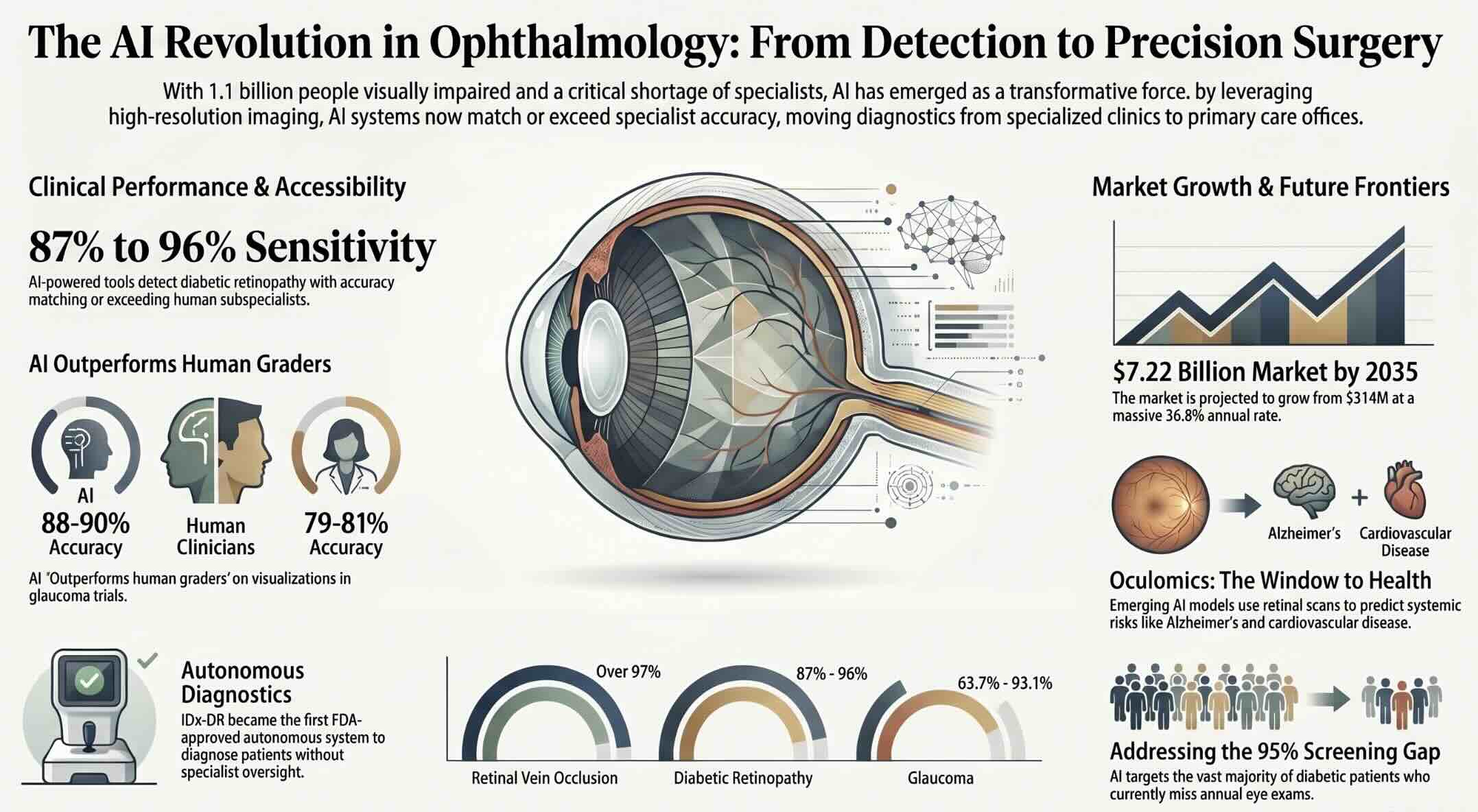
IDx-DR became the first FDA-approved autonomous AI diagnostic system in 2018, detecting diabetic retinopathy with 87.2% sensitivity and 90.7% specificity across 900 patients in primary care settings.
How accurate is AI in detecting eye diseases?
Deep learning algorithms achieve 88% to 96% sensitivity in detecting diabetic retinopathy and area-under-the-curve values around 0.95 for glaucoma detection, matching or exceeding subspecialist performance in prospective clinical trials.
Key Takeaways
- The Society for Artificial Intelligence in Vision and Ophthalmology was established in May 2025 as the first global organization dedicated to advancing AI integration in clinical eye care.
- AI-powered diagnostic tools like IDx-DR and EyeArt detect diabetic retinopathy with sensitivity rates between 87% and 96%, enabling autonomous screening in primary care offices without specialist oversight.
- Deep learning systems analyzing fundus photographs and OCT volumes for glaucoma routinely achieve area-under-the-curve values around 0.95, matching or exceeding subspecialist performance in clinical tests.
- The global AI in ophthalmology market is projected to grow from $430.43 million in 2026 to $7.22 billion by 2035, driven by rising eye disease prevalence and expanding tele-ophthalmology services.
Table of contents
- Introduction
- Key Questions
- Key Takeaways
- Impact of AI in ophthalmology
- How AI in Ophthalmology Changes Clinical Practice
- Why Eye Care Is Uniquely Suited for AI Integration
- Detecting Diabetic Retinopathy with Autonomous AI Systems
- AI-Powered Glaucoma Diagnosis Through Deep Learning
- Age-Related Macular Degeneration and Predictive AI Models
- Bringing AI Screening to Primary Care Offices
- Computer Vision at the Heart of Retinal Image Analysis
- Robotic Surgery and AI-Guided Precision in Eye Procedures
- Personalizing Treatment Through Machine Learning
- Tele-Ophthalmology Powered by Remote AI Screening
- FDA-Approved AI Devices Reshaping Ophthalmic Diagnostics
- Confronting Bias and Data Quality in Ophthalmic AI
- Preparing Clinicians for an AI-Integrated Future
- The Expanding Global Market for AI in Eye Care
- Ethical Dimensions of AI-Driven Eye Diagnostics
- Pediatric Eye Care and Emerging AI Applications
- Navigating Regulatory and Validation Hurdles
- Where AI in Ophthalmology Is Heading Next
- Key Insights
- Real-World Examples
- Case Studies
- Frequently Asked Questions
Impact of AI in ophthalmology
The impact of artificial intelligence in ophthalmology is truly substantial. Evidence confirms AI can improve patient access to clinical screening, diagnosis and also reduce costs, particularly in high-risk groups.
A paper from the International Journal of Ophthalmology found that, compared to clinical grading, the sensitivity and accuracy of AI to detect eye diseases was the following:
- Age-related macular degeneration – 75% to 100%
- Cataract – over 70%
- Glaucoma – 63.7% to 93.1%
- Non-proliferative diabetic retinopathy – 75% to 94.7%
- Proliferative diabetic retinopathy – 75% to 91%
- Retinal vein occlusion – over 97%
- Retinopathy of prematurity – over 95%
The full impact of AI in ophthalmology requires further research, but one of the most recent papers on this topic revealed its implementation could be fully and semi-automated. The fully automated AI model would work without any human involvement. Artificial intelligence would be able to initiate referrals to ophthalmologists appointments when necessary. It could also determine which patients are suitable for community-based monitoring. On the other hand, the semi-automated AI model works with human involvement in different ways, which only serves to enhance classification made by deep learning. The AI technology would be able to fill all the gaps in the screening process and thereby prove to be a cost-effective solution in ophthalmology.
How AI in Ophthalmology Changes Clinical Practice
Artificial intelligence in ophthalmology refers to the application of machine learning, deep learning, and computer vision algorithms to analyze ophthalmic imaging data and clinical records for diagnostic and therapeutic purposes. These systems process retinal photographs, OCT scans, visual field tests, and slit-lamp images to identify patterns that indicate disease presence, severity, or progression risk. The technology operates across a spectrum from decision-support tools that assist clinicians to fully autonomous systems that deliver diagnostic results without human oversight.
Why Eye Care Is Uniquely Suited for AI Integration
Ophthalmology generates more standardized, high-resolution digital imaging data than nearly any other medical specialty, making it an ideal field for training AI algorithms. Fundus photography, optical coherence tomography, visual field testing, and anterior segment imaging all produce structured datasets with consistent formatting and measurable features. These imaging modalities capture detailed anatomical information about the retina, optic nerve, macula, and cornea in formats that deep learning models can process with remarkable precision. The reliance on image-based diagnosis means that the core clinical task aligns directly with the strengths of convolutional neural networks and other computer vision architectures. Ophthalmology also benefits from well-defined disease classification systems that provide clear training labels for supervised machine learning models. Conditions like diabetic retinopathy follow established grading scales that enable researchers to build large, consistently labeled training datasets from clinical archives spanning decades of patient care. The combination of abundant imaging data and standardized disease classifications has made ophthalmology one of the most productive fields for AI-driven diagnostics in all of medicine.
The second factor driving AI adoption in ophthalmology is the severe global shortage of trained eye care specialists relative to the growing burden of preventable blindness. Over 592 million cases of diabetic retinopathy are projected by 2025, yet many regions lack sufficient ophthalmologists to screen even a fraction of the at-risk population. Rural communities in developing nations may have only one ophthalmologist serving hundreds of thousands of people, creating diagnostic bottlenecks that allow treatable conditions to progress to irreversible vision loss. AI screening systems deployed in primary care offices, community clinics, and mobile health units can bridge this gap by bringing specialist-level diagnostic capability to settings where no specialist exists. This democratization of eye care represents one of the most socially impactful applications of artificial intelligence in the healthcare sector. Primary care physicians and nurses can operate AI-powered retinal cameras after minimal training, enabling population-scale screening programs that were previously impossible without armies of trained ophthalmologists.
Detecting Diabetic Retinopathy with Autonomous AI Systems
Diabetic retinopathy remains the leading cause of preventable blindness among working-age adults, affecting millions of people with diabetes who require regular retinal screening to catch the disease before it destroys their vision. Traditional screening relies on trained ophthalmologists or certified graders reviewing fundus photographs, a process that creates enormous bottlenecks given the growing diabetes epidemic worldwide. AI systems have demonstrated the ability to detect diabetic retinopathy autonomously, without requiring a human specialist to review each image before delivering a clinical result. The IDx-DR system, now known as LumineticsCore, became the first FDA-approved autonomous AI diagnostic device in any field of medicine when it received clearance in 2018. It achieved 87.2% sensitivity and 90.7% specificity for detecting more than mild diabetic retinopathy across a pivotal trial of 900 patients at ten primary care sites. This landmark approval proved that AI could deliver specialty-level eye disease diagnostics in primary care settings where no ophthalmologist is present. The system analyzes retinal photographs captured by a standard fundus camera and provides either a positive or negative result within minutes.
Competing systems have since pushed accuracy rates even higher through advances in deep learning architecture and training data quality. EyeArt, developed by Eyenuk, demonstrated 96% sensitivity and 88% specificity for detecting more than mild diabetic retinopathy in a study of 942 individuals with diabetes. For vision-threatening diabetic retinopathy specifically, EyeArt achieved 97% sensitivity and 90% specificity, making it one of the most accurate screening tools available for the most dangerous forms of the disease. AEYE Health reported sensitivity of 93% and specificity of 91.4% on desktop cameras, with comparable performance on handheld devices that enable screening in remote locations. These systems require no pre-programming of patient demographics or disease history and can grade retinal images in seconds. The speed and accuracy of autonomous AI screening allows clinics to process dozens of patients per hour compared to the handful that a human grader could evaluate in the same timeframe. Each platform uses deep learning models trained on hundreds of thousands of labeled retinal images to recognize the microaneurysms, hemorrhages, and exudates that characterize diabetic eye disease.
Despite these impressive performance metrics, real-world adoption of AI-based diabetic retinopathy screening has remained surprisingly low in the United States. A recent cohort study published in JAMA Ophthalmology found that less than 5% of diabetic patients received ophthalmic imaging for diabetic retinopathy from 2019 to 2023. Among those patients who were screened, only a small fraction underwent AI-based screening despite its demonstrated advantages in sensitivity and referral rates for OCT imaging. Regional and demographic disparities in AI imaging use highlight persistent barriers to adoption, including limited awareness among primary care providers, cost concerns, and challenges integrating AI tools into existing clinical workflows. Less than two-thirds of patients with type 1 or type 2 diabetes undergo an annual eye examination as recommended by clinical guidelines, representing an enormous unmet need that AI screening could address. The gap between demonstrated AI capability and actual clinical deployment remains one of the most significant challenges facing the field of ophthalmic artificial intelligence today.
The reimbursement landscape for AI-based diabetic retinopathy screening took an important step forward with the introduction of Current Procedural Terminology code 92229 in January 2021. This billing code allows providers to receive payment specifically for AI-based retinal screening services, reducing one of the key financial barriers that previously limited adoption. Despite the availability of this reimbursement mechanism, tracking data shows that utilization remains concentrated in a small number of health systems and geographic regions. Expanding adoption will require coordinated efforts across medical education, insurance coverage policies, and workflow integration support from AI vendors. The potential to prevent blindness in millions of people makes solving the adoption challenge one of the most urgent priorities in AI healthcare implementation.
AI in Ophthalmology Explorer
Select a condition to explore how AI is transforming detection, accuracy, and patient outcomes in eye care. Compare AI performance against human specialists.
AI-Powered Glaucoma Diagnosis Through Deep Learning
Beyond diabetic retinopathy screening, AI is making substantial progress in detecting glaucoma, a disease that remains the leading cause of irreversible blindness globally with projections suggesting it will affect over 111 million individuals by 2040. Glaucoma is particularly dangerous because it progresses silently, destroying peripheral vision before patients notice any symptoms. By the time patients present with noticeable vision loss, significant and permanent optic nerve damage has already occurred, making early detection through screening programs essential for preserving sight. Deep learning systems analyzing fundus photographs and OCT volumes have demonstrated remarkable diagnostic accuracy for glaucoma. A meta-analysis of 48 studies found that deep learning algorithms achieved pooled sensitivity of 92% and specificity of 93% using fundus photography, with an area-under-the-curve of 0.90. For OCT-based detection, pooled sensitivity reached 90% with specificity of 87%, confirming strong performance across both major imaging modalities used in clinical practice.
Research from the University College London Institute of Ophthalmology and Moorfields Eye Hospital compared AI algorithm performance against human graders across 6,304 fundus images. The algorithm correctly identified glaucoma patients in 88% to 90% of cases, compared to 79% to 81% accuracy from experienced human graders. This performance gap demonstrates that AI systems can outperform trained human experts in specific diagnostic tasks when given standardized imaging inputs. Sequence-aware models have taken glaucoma AI beyond simple diagnosis into the realm of disease progression prediction. These advanced systems can detect visual field worsening up to 1.7 years earlier than conventional linear trend analyses, giving clinicians a critical head start in adjusting treatment before significant vision loss occurs. AI models integrating OCT, visual field data, and clinical information have predicted the need for incisional glaucoma surgery with an area-under-the-curve of 0.92, enabling more proactive surgical planning. The application of computer vision in medical imaging continues to push the boundaries of what automated analysis can achieve in complex diagnostic scenarios.
The potential impact of AI glaucoma detection extends far beyond individual patient encounters to population-level public health screening. Traditional glaucoma screening requires specialized equipment, trained technicians, and ophthalmologist interpretation, creating a bottleneck that limits screening coverage in most countries. AI-powered screening could enable community health workers to capture fundus photographs using portable cameras and receive instant risk assessments without waiting for specialist review. This approach would be particularly valuable in regions of Africa, South Asia, and rural communities worldwide where the ratio of ophthalmologists to population makes comprehensive screening virtually impossible through traditional methods. Addressing glaucoma at a population scale requires the kind of automated, scalable diagnostic infrastructure that only AI can provide at current technology costs.
Age-Related Macular Degeneration and Predictive AI Models
The success of AI in diabetic retinopathy and glaucoma detection has opened pathways for similar applications in age-related macular degeneration, a condition expected to affect nearly 20 million Americans by 2030. AMD is the leading cause of central vision loss in people over 50, and its progression can be slowed with early treatment but cannot be reversed once advanced stages develop. AI systems analyze OCT scans and fundus photographs to detect the drusen deposits, pigmentary changes, and fluid accumulations that characterize different AMD stages with accuracy that approaches and sometimes exceeds clinical expert performance. Deep learning models built on architectures like U-Net++ can segment retinal layers and identify subretinal fluid, intraretinal fluid, and pigment epithelial detachment in OCT images with high precision. These automated segmentation tools reduce the time ophthalmologists spend analyzing individual scans from minutes to seconds, enabling more efficient patient throughput in busy retinal practices. Moorfields Eye Hospital and the UCL Institute of Ophthalmology have developed AI systems specifically designed to simplify recruitment for geographic atrophy clinical trials by automatically identifying eligible patients from routine imaging data.
Predictive AI models for AMD go beyond simple diagnosis to forecast how individual patients’ conditions will evolve over time based on their current imaging features and clinical history. These models analyze subtle patterns in OCT scans that are invisible to the human eye but correlate strongly with future disease progression trajectories. By identifying patients at highest risk of rapid deterioration, AI enables ophthalmologists to prioritize treatment initiation and schedule follow-up appointments at intervals matched to each patient’s specific risk profile. This personalized approach to AMD management contrasts sharply with the one-size-fits-all scheduling protocols that most clinics currently follow.
Bringing AI Screening to Primary Care Offices
The shift of AI screening from specialty ophthalmology clinics into primary care offices represents one of the most significant deployment strategies for reaching patients who would otherwise never receive timely eye examinations. Primary care providers see diabetic patients regularly for blood glucose management, medication adjustments, and routine health maintenance visits, creating natural touchpoints for integrating retinal screening into existing clinical workflows. AI-powered retinal cameras designed for primary care use can be operated by medical assistants after just a few hours of training, eliminating the need for specialized ophthalmic technicians. The cameras capture retinal images through undilated pupils in many cases, reducing patient discomfort and visit length compared to traditional dilated eye examinations. Patients who screen positive receive immediate referrals to ophthalmology specialists, while those with negative results receive documentation of their screening that satisfies annual eye examination requirements. Deploying AI screening at the point of primary care contact eliminates the most common barrier to diabetic eye screening, which is the need for patients to schedule and attend a separate appointment with an eye specialist. The impact of automation in healthcare extends well beyond efficiency gains to fundamental improvements in patient access and disease prevention outcomes.
The integration of AI screening into primary care workflows requires careful attention to implementation factors that determine whether the technology delivers on its promise in real clinical settings. Camera placement, lighting conditions, staff training protocols, and electronic health record integration all influence the quality of captured images and the percentage of patients who receive conclusive results. Facilities that invest in dedicated screening spaces with controlled lighting achieve higher image quality rates than those that attempt to capture retinal photographs in standard examination rooms. Workflow integration must ensure that AI screening results flow seamlessly into patient records, trigger appropriate referral pathways, and generate billing documentation for reimbursement processing. The experience of early adopters shows that successful primary care AI screening programs require champion physicians who advocate for the technology within their practice groups.
Studies tracking primary care AI screening deployments have revealed that patients screened through AI systems receive referrals for OCT imaging at higher rates than those evaluated through traditional methods. This increased referral rate reflects the AI system’s ability to detect subtle abnormalities that non-specialist providers might miss during brief fundus examinations. The higher detection rate translates directly into earlier treatment initiation for patients with vision-threatening conditions, potentially preventing thousands of cases of avoidable blindness annually. Expanding primary care AI screening to all diabetes management practices across the United States alone could reach millions of patients who currently fall through gaps in the eye care system.
Computer Vision at the Heart of Retinal Image Analysis
Computer vision provides the technical foundation for every AI application in ophthalmology, translating raw pixel data from retinal images into clinically meaningful diagnostic information. Modern ophthalmic AI systems use convolutional neural networks that have been trained on millions of labeled images to recognize the visual features associated with specific eye diseases and their severity stages. These networks learn hierarchical representations of image features, progressing from simple edge and texture detectors in early layers to complex disease-specific pattern recognizers in deeper layers. The training process requires carefully curated datasets where expert ophthalmologists have annotated each image with disease labels, severity grades, and anatomical landmarks. Transfer learning techniques allow models pre-trained on large general image datasets to be fine-tuned for ophthalmic applications using relatively smaller clinical datasets. The ability to apply transfer learning from general image recognition to specialized medical imaging has dramatically reduced the data requirements and training time for developing clinically useful ophthalmic AI systems. Image preprocessing steps including color normalization, contrast enhancement, and artifact removal ensure consistent input quality regardless of the camera model or capture conditions used at different clinical sites.
Beyond basic disease classification, advanced computer vision techniques enable detailed anatomical segmentation that quantifies disease burden at a level of precision impossible through manual measurement. AI systems can segment individual retinal layers in OCT volumes, measure nerve fiber layer thickness changes of a few micrometers, and track the exact boundaries of fluid pockets or lesions across serial imaging sessions. This quantitative capability transforms ophthalmic imaging from a qualitative assessment tool into a precise measurement instrument. The ability to detect and measure changes smaller than what the human eye can perceive provides ophthalmologists with objective biomarkers for tracking disease progression and treatment response. Automated segmentation also eliminates the inter-observer variability that plagues manual measurements, where different graders may disagree on the exact boundaries of a lesion or the precise thickness of a retinal layer.
The latest frontier in ophthalmic computer vision involves multimodal models that integrate data from multiple imaging sources to produce more comprehensive diagnostic assessments than any single modality can achieve alone. These models combine information from fundus photography, OCT, visual field testing, and anterior segment imaging to create holistic patient profiles that capture both structural and functional aspects of eye disease. Integrating multiple data streams mirrors the clinical reasoning process of experienced ophthalmologists who synthesize information from diverse examinations before reaching diagnostic conclusions. Understanding how data augmentation works is essential for appreciating how researchers expand limited clinical datasets to train these complex multimodal architectures effectively.
Robotic Surgery and AI-Guided Precision in Eye Procedures
AI is transforming ophthalmic surgery through tools that enhance precision, reduce human error, and optimize outcomes for procedures ranging from routine cataract removal to complex retinal interventions. Cataract surgery is the most frequently performed surgical procedure in the world, and its standardized nature makes it particularly suitable for AI-assisted analysis, planning, and guidance. AI-driven preoperative screening programs can analyze slit lamp photographs and OCT images to identify cataract severity with accuracy rates of 90% or higher, automating triage decisions that currently require specialist evaluation. The ALLY Adaptive Cataract Treatment System uses AI to predictively locate iris anatomical markers for confident iris registration, accounting for cyclotorsion and ensuring precise corneal incision placement and astigmatic correction. This AI-driven approach eliminates manual marking, which has long been a common source of human error in refractive cataract surgery procedures. The system also uses AI densitometry to adjust fragmentation patterns based on lens morphology and cataract density in real time, optimizing each procedure for the specific characteristics of the individual patient’s eye.
The role of AI in surgical planning extends beyond intraoperative guidance to encompass the complex calculations required for selecting and positioning intraocular lenses that will determine the patient’s visual outcome for the rest of their life. Traditional IOL power calculations rely on formulas that use measurements of corneal curvature, axial length, and anterior chamber depth to predict the lens power needed for a desired refractive outcome. AI-powered tools like CustomLens AI incorporate advanced algorithms that guide surgeons through the complexities of premium lens selection, considering spherical correction, toric correction for astigmatism, and presbyopia-correcting options simultaneously. These systems analyze complex diagnostic data and suggest optimal surgical parameters with greater speed and precision than manual calculation methods. By reducing the expertise barrier for premium lens selection, AI tools are expanding patient access to advanced visual outcomes that were previously available only from the most experienced refractive surgeons.
AI analysis of surgical video recordings represents an emerging application that could transform how surgeons learn, train, and maintain quality standards throughout their careers. Deep learning algorithms can identify and segment individual surgical phases in cataract surgery videos, measure instrument movements, and detect deviations from standard technique that correlate with increased complication risk. This automated video analysis creates objective performance metrics that supplement the subjective assessments traditionally used in surgical training and credentialing. The technology enables personalized feedback loops where surgeons can review their own technique analyzed by AI algorithms that have learned from thousands of procedures performed by expert surgeons. The history of robotic surgery shows a clear trajectory toward increasing integration of AI-powered decision support with physical surgical execution.
Looking ahead, the integration of digital twin technology with AI surgical planning could enable ophthalmologists to simulate procedures virtually before touching the patient’s eye. Digital twin models of individual eyes would incorporate biometric measurements, tissue properties, and disease characteristics to predict how specific surgical interventions will affect visual outcomes. Surgeons could test multiple approaches in the virtual environment and select the strategy most likely to produce the optimal result before entering the operating room. This simulation capability would be particularly valuable for complex cases where surgical decisions involve significant trade-offs between competing clinical objectives.
Personalizing Treatment Through Machine Learning
Machine learning models are enabling ophthalmologists to move beyond standardized treatment protocols toward truly personalized care plans tailored to each patient’s unique disease characteristics, genetics, and predicted response patterns. For wet age-related macular degeneration, AI algorithms analyze OCT imaging features to predict which patients will respond best to specific anti-VEGF injection regimens, potentially reducing the number of unnecessary treatments while maintaining visual outcomes. These predictive models identify biomarkers in retinal fluid patterns, pigment epithelium morphology, and photoreceptor layer integrity that correlate with treatment response trajectories over time. Patients predicted to maintain stability on extended treatment intervals can be scheduled less frequently, reducing the burden of monthly clinic visits and injection procedures. Conversely, patients identified as high-risk for rapid deterioration can receive intensified monitoring and treatment before irreversible vision loss occurs. The vision of personalized screening with artificial intelligence applies directly to eye care, where individual disease trajectories vary enormously even among patients with the same clinical diagnosis.
Pharmacogenomic AI models represent the next frontier in personalized ophthalmic treatment by incorporating genetic information alongside imaging and clinical data to predict drug response. Certain genetic variants influence how patients metabolize anti-VEGF drugs, respond to glaucoma medications, or heal after surgical procedures. By integrating genomic data with treatment outcome databases, machine learning models can identify genotype-phenotype correlations that inform more precise prescribing decisions. The challenge lies in assembling sufficiently large, diverse datasets that include both genetic profiles and longitudinal treatment outcomes, a resource-intensive effort that requires collaboration across multiple institutions and health systems. Several academic medical centers and industry consortia are building the data infrastructure needed to make pharmacogenomic AI a clinical reality in ophthalmology within the next decade.
Tele-Ophthalmology Powered by Remote AI Screening
The expansion of tele-ophthalmology services accelerated dramatically during the COVID-19 pandemic, and AI-powered remote screening has become a permanent feature of many eye care delivery models. Tele-ophthalmology combines portable imaging devices with cloud-based AI analysis to deliver eye disease screening in locations where patients cannot easily travel to see an ophthalmologist. Community health workers in rural India, sub-Saharan Africa, and remote island nations can capture retinal images using smartphone-based adapters or portable fundus cameras and upload them for instant AI analysis. The AI system returns a screening result within minutes, enabling immediate triage decisions about which patients need urgent specialist referral versus routine follow-up. This remote screening model has the potential to reach hundreds of millions of people in low-resource settings where the nearest ophthalmologist may be hundreds of miles away. The approach aligns with the broader trend of bringing AI into healthcare business processes to improve efficiency and expand access beyond traditional clinic walls.
The technical infrastructure supporting tele-ophthalmology AI has matured significantly, with 5G connectivity and edge computing enabling faster image transmission and processing in areas with limited internet bandwidth. Cloud-based AI platforms can process images uploaded from thousands of screening sites simultaneously, providing scalable diagnostic capacity that grows with program demand rather than requiring proportional increases in specialist staffing. Data security and patient privacy protections must be robust, particularly in cross-border screening programs where images may traverse multiple jurisdictions with different data protection regulations. The role of healthcare documentation becomes critical in tele-ophthalmology, where clear records must link screening results to patient identities and ensure seamless handoffs to treating physicians.
Mobile health applications that incorporate AI-powered self-screening represent a consumer-facing extension of tele-ophthalmology that could further expand access to basic eye health assessment. Several startups have developed smartphone applications that use the device’s camera and flash to capture crude fundus images or assess visual function through interactive tests. While these consumer applications currently lack the accuracy of clinical-grade AI screening systems, rapid improvements in smartphone camera quality and computational power are narrowing the gap. The regulatory pathway for consumer eye health AI applications remains uncertain, with agencies balancing the potential public health benefit of wider screening access against the risks of false reassurance from inaccurate results.
FDA-Approved AI Devices Reshaping Ophthalmic Diagnostics
The FDA approval pathway for AI-based ophthalmic diagnostic devices has established a regulatory framework that balances innovation speed with patient safety requirements. IDx-DR set the benchmark when it received FDA authorization in 2018 as the first autonomous AI diagnostic system in any field of medicine, demonstrating that AI could meet the rigorous evidentiary standards required for clinical deployment. The FDA requires all subsequent autonomous diabetic retinopathy screening algorithms to demonstrate performance equivalent to IDx-DR in prospective studies with diverse patient cohorts. This benchmark approach provides clarity for developers about the performance thresholds they must achieve while ensuring that new systems maintain at least the safety and accuracy standards established by the first approved device. Several additional systems have since received FDA clearance, including EyeArt from Eyenuk and devices from AEYE Health, creating a competitive market that drives continued improvement. The existence of multiple FDA-approved autonomous AI diagnostic tools for a single condition represents a milestone in medical AI that few other specialties have achieved. Regulatory approval signals to health systems, insurers, and patients that these technologies have met objective standards for clinical reliability.
The classification of AI diagnostic devices within the FDA’s regulatory framework determines the level of evidence required for approval and the post-market surveillance obligations that manufacturers must fulfill. Most autonomous AI screening devices are classified as Class II medical devices requiring the De Novo regulatory pathway, which involves clinical performance testing but does not require the full premarket approval process mandated for Class III devices. This classification reflects the moderate risk profile of screening tools that identify patients needing further evaluation rather than making final treatment decisions. Post-market surveillance requirements ensure that manufacturers continue monitoring device performance in real-world clinical settings after initial approval, capturing data on accuracy rates across diverse patient populations and imaging conditions.
The regulatory landscape is evolving to accommodate more sophisticated AI applications that go beyond simple screening to encompass disease progression prediction, treatment recommendation, and surgical planning support. These more complex applications may require different regulatory approaches because they influence clinical decision-making in ways that simple pass-fail screening tools do not. Regulators are developing frameworks for evaluating AI systems that continuously learn and update their algorithms based on new clinical data, a characteristic that traditional regulatory approval processes were not designed to accommodate. The balance between enabling rapid innovation and maintaining patient safety will shape the pace and direction of AI deployment in ophthalmology for years to come.
Confronting Bias and Data Quality in Ophthalmic AI
Algorithmic bias in ophthalmic AI systems represents a critical challenge that threatens to perpetuate or amplify existing disparities in eye care access and outcomes across racial, ethnic, and socioeconomic groups. AI models are only as representative as the data on which they are trained, and many landmark ophthalmic AI datasets overrepresent patients from high-income countries, urban academic medical centers, and specific racial demographics. A model trained predominantly on fundus photographs from patients of European descent may perform less accurately when screening patients with darker fundus pigmentation, potentially resulting in higher false-negative rates in the populations that already face the greatest barriers to eye care access. The generalizability challenge is compounded by differences in imaging equipment, camera settings, and image quality across clinical sites, which can introduce systematic biases that the AI model learns to associate with diagnostic predictions. Ensuring that ophthalmic AI systems perform equitably across all patient populations requires deliberate investment in diverse training datasets and rigorous validation across demographic subgroups. The broader question of whether AI risks outweigh benefits applies directly to ophthalmic AI when biased systems could worsen health disparities rather than reducing them.
Data quality challenges extend beyond demographic representation to encompass the accuracy and consistency of the disease labels used to train supervised learning models. Disagreement among expert graders on disease severity classification introduces noise into training data that can limit model performance ceilings. Different grading protocols used at different institutions create inconsistencies that make it difficult to combine datasets for training larger, more powerful models. Image quality variation across camera types, patient cooperation levels, and capture conditions adds another dimension of noise that models must learn to accommodate. Addressing these data quality issues requires sustained investment in standardized grading protocols, quality control procedures, and multi-institutional data sharing agreements that enable the creation of representative, well-annotated training datasets.
Preparing Clinicians for an AI-Integrated Future
The integration of AI into ophthalmic practice requires fundamental changes in how ophthalmologists are trained, from medical school through residency and into continuing education throughout their careers. Current medical education curricula rarely include instruction on AI fundamentals, data science concepts, or the critical evaluation skills needed to assess whether a particular AI tool is appropriate for use in a specific clinical context. Residents who graduate without understanding how AI algorithms are developed, validated, and deployed will struggle to effectively incorporate these tools into their clinical decision-making or to identify situations where AI recommendations should be questioned or overridden. The Society for Artificial Intelligence in Vision and Ophthalmology, established in May 2025, aims to provide a platform for sharing research, establishing consensus standards, and fostering education in ophthalmic AI. Medical schools and residency programs that proactively integrate AI literacy into their curricula will produce graduates better prepared for the technology-rich practice environments that will define ophthalmology in the coming decades. Training programs must equip future ophthalmologists not just to use AI tools but to understand their limitations, recognize their failure modes, and maintain the clinical judgment needed to override AI recommendations when appropriate.
Beyond physician training, the AI transformation of ophthalmology creates new roles and skill requirements for ophthalmic technicians, nurses, and administrative staff who support clinical operations. Technicians must learn to operate AI-powered imaging devices, troubleshoot technical issues, and ensure that image capture quality meets the standards required for reliable AI analysis. Nurses and medical assistants in primary care settings need training on AI screening protocols, result interpretation, and patient communication about what AI screening results mean for their ongoing care. Administrative staff must navigate new billing codes, insurance authorization requirements, and data management procedures associated with AI diagnostic services. The workforce development challenge spans the entire healthcare team, not just the physicians who ultimately make clinical decisions. Programs that develop comprehensive training approaches across all staff roles achieve smoother AI integration and higher overall screening quality than those focusing exclusively on physician education.
The continuing education dimension is particularly important because AI technology evolves rapidly and clinicians must stay current with new capabilities, updated algorithms, and emerging evidence about AI system performance in clinical practice. Professional societies, device manufacturers, and academic medical centers all play roles in providing ongoing education about AI tools and their appropriate clinical applications. Peer-reviewed publications from journals like the new Artificial Intelligence in Vision and Ophthalmology provide a venue for clinicians to access the latest research and contribute their own clinical experience with AI integration. The study of machine learning fundamentals gives clinicians the conceptual framework needed to evaluate AI claims critically rather than accepting vendor marketing at face value.
The Expanding Global Market for AI in Eye Care
The global AI in ophthalmology market is experiencing explosive growth as clinical validation data accumulates, regulatory pathways mature, and health systems worldwide recognize the potential for AI to address critical gaps in eye care delivery. Market valuations vary across research firms, but multiple analyses converge on projecting compound annual growth rates exceeding 25% through the early 2030s, with some estimates reaching 36.8% CAGR through 2035. North America currently dominates the market with approximately 51% of global revenue, driven by regulatory clarity, established reimbursement mechanisms, and strong academic-industry collaboration networks. The diabetic retinopathy detection segment accounts for the largest share at approximately 28.7% of the market, reflecting the relative maturity and clinical validation of AI screening tools for this condition. Deep learning technology drives 36.8% of market revenue by segment, confirming its position as the dominant technical approach for ophthalmic AI applications. The Asia Pacific region is emerging as the fastest-growing market for AI in ophthalmology, driven by massive diabetic populations, rapidly aging demographics, and government investments in healthcare technology infrastructure. Investment in healthtech startups specializing in AI-powered diagnostics continues to attract venture capital across both established and emerging markets.
The competitive landscape features a mix of established medical device companies, technology giants, and specialized AI startups competing across different segments of the market. Major players include Google, which developed a diabetic retinopathy screening system through its DeepMind Health division, along with established ophthalmic device manufacturers like Zeiss, Topcon, and Nidek that are integrating AI capabilities into their existing imaging platforms. Specialized AI companies including Eyenuk, Digital Diagnostics, AEYE Health, and Altris AI focus exclusively on ophthalmic AI applications and often move faster than larger companies in bringing new algorithms to clinical validation. Strategic partnerships between AI developers and hospital systems provide the clinical data access and real-world testing environments needed to refine algorithms for commercial deployment. In May 2025, Topcon Healthcare acquired RetInSight GmbH to strengthen its AI-driven ophthalmic diagnostic capabilities, illustrating the consolidation trend reshaping the market.
The formation of Cascader Limited in May 2025, a joint venture between Moorfields Eye Hospital, UCL Institute of Ophthalmology, and Topcon Healthcare, represents a new model for translating academic AI research into commercial clinical tools. This partnership combines the research strengths and clinical datasets of one of the world’s leading eye hospitals with the manufacturing and distribution capabilities of a global ophthalmic device company. The venture aims to commercialize AI-driven oculomics, a field that uses retinal imaging data to detect systemic health conditions beyond traditional eye diseases. Retinal blood vessels and neural tissue provide windows into cardiovascular health, neurological conditions, and metabolic disorders that AI can potentially identify from routine eye examinations. This expansion of ophthalmic AI beyond eye disease into general health screening could dramatically increase the addressable market and clinical impact of retinal imaging technology.
Market growth projections must be tempered by realistic assessments of the barriers to adoption that have slowed AI deployment in many health systems despite strong evidence of clinical benefit. Reimbursement policies in many countries still do not adequately compensate providers for AI-based screening services, reducing the financial incentive to invest in equipment and training. Integration with existing electronic health records and clinical workflow systems remains technically challenging and requires custom development work for each health system. Resistance from clinicians who view AI as threatening to their professional autonomy or who distrust algorithmic decision-making creates adoption friction that no amount of clinical evidence alone can overcome. Overcoming these barriers will require coordinated action across regulators, payers, technology developers, and clinical leadership to create the conditions for widespread AI adoption in eye care.
Ethical Dimensions of AI-Driven Eye Diagnostics
The ethical implications of deploying AI in ophthalmic diagnosis span questions of patient consent, data ownership, algorithmic accountability, and the potential for AI to either reduce or amplify existing inequities in eye care access. Patients undergoing AI-based screening may not fully understand that their retinal images are being analyzed by an algorithm rather than a human specialist, raising questions about whether current consent processes adequately inform patients about the nature of their diagnostic encounter. Data ownership becomes complex when images captured in primary care settings are transmitted to cloud-based AI platforms operated by commercial companies, with questions about who controls the data, how long it is retained, and whether it can be used for algorithm development or sold to third parties. Algorithmic accountability presents a novel ethical challenge because when an AI system produces an incorrect diagnosis, the chain of responsibility among the device manufacturer, the software developer, the deploying institution, and the supervising clinician remains unclear in most jurisdictions. The discussion of cognitive insight and artificial intelligence helps frame these ethical questions within the broader context of how AI systems make and communicate diagnostic decisions.
The equity implications of ophthalmic AI are particularly acute because the populations most in need of expanded screening access are often the same populations most vulnerable to algorithmic bias and least empowered to advocate for their interests in technology design processes. If AI screening systems perform less accurately for patients from underrepresented racial or ethnic groups, deploying these systems at scale could create a false sense of progress while actually widening health disparities. Ethical AI deployment requires transparent reporting of performance metrics disaggregated by demographic subgroups, active monitoring for disparate outcomes in deployed systems, and ongoing investment in improving performance for populations where accuracy falls below acceptable thresholds. The tension between moving quickly to deploy life-saving screening technology and taking the time needed to ensure equitable performance creates a genuine ethical dilemma that does not have a simple resolution.
Pediatric Eye Care and Emerging AI Applications
AI applications in pediatric ophthalmology represent a growing area of research that addresses unique challenges in detecting and treating eye conditions in children who cannot always communicate visual symptoms or cooperate with standard examination techniques. Retinopathy of prematurity, a potentially blinding condition affecting premature infants, requires regular screening by specialized pediatric ophthalmologists during the critical weeks after birth. AI systems that analyze wide-field retinal images of premature infants can identify cases requiring treatment with accuracy approaching that of expert retinal specialists, potentially enabling screening in neonatal intensive care units that lack on-site ophthalmic expertise. Amblyopia detection in young children represents another promising AI application, as early identification and treatment during the critical period of visual development can prevent permanent visual impairment. AI-powered visual acuity testing tools designed for preverbal children use eye-tracking technology and preferential looking paradigms to assess visual function without requiring the child to read letters on a chart. Strabismus assessment through AI analysis of facial photographs could enable population-scale screening for eye alignment disorders during routine pediatric wellness visits.
The challenges of developing AI for pediatric ophthalmology include the relative scarcity of labeled training data compared to adult eye diseases, the rapid anatomical changes that occur in developing eyes, and the need for imaging protocols adapted to uncooperative young patients. Pediatric retinal images look fundamentally different from adult images due to ongoing myelination, smaller globe dimensions, and the specific vascular patterns associated with developing eyes. Models trained exclusively on adult data may perform poorly when applied to pediatric populations, requiring dedicated pediatric training datasets that are expensive and time-consuming to assemble. Institutional review board requirements for research involving children add complexity to data collection efforts and limit the pace at which pediatric ophthalmic AI can be developed and validated. Despite these challenges, the potential to prevent childhood blindness through AI-enabled early detection justifies sustained investment in this emerging field.
AI is also being explored for screening refractive errors in school-age children, a condition that affects learning, social development, and quality of life when uncorrected. Automated refraction devices powered by AI algorithms can estimate prescription needs in seconds, enabling efficient screening of entire classrooms during school health programs. The ability to detect disease through AI testing has expanded from cardiology to ophthalmology, with similar principles of rapid automated analysis being applied across medical specialties. Children identified with significant refractive errors through AI screening can be referred immediately for comprehensive eye examinations and prescription eyeglasses, closing the gap between detection and treatment that allows many children to struggle academically for years before receiving needed vision correction.
Navigating Regulatory and Validation Hurdles
The path from AI algorithm development to clinical deployment in ophthalmology involves navigating regulatory requirements, clinical validation standards, and post-market surveillance obligations that vary significantly across different countries and health systems. Developers must demonstrate not only that their algorithms achieve high accuracy on curated test datasets but that they maintain performance when deployed in real-world clinical settings with diverse patient populations, variable image quality, and different imaging equipment. The gap between laboratory performance and real-world effectiveness, often called the external validation challenge, has tripped up many promising AI systems that performed well in controlled research settings but faltered when encountering the messiness of routine clinical practice. Internal validation datasets consistently show higher accuracy than external validation datasets in meta-analyses of ophthalmic AI performance, highlighting the importance of independent testing on data the algorithm has never encountered during training or tuning. Regulatory agencies are increasingly requiring multi-site, prospective validation studies that assess AI performance across diverse clinical environments before granting approval. The requirement for prospective clinical trials raises the cost and timeline for bringing ophthalmic AI products to market, creating barriers for smaller startups that may have developed promising algorithms but lack the resources for large-scale clinical testing.
The challenge of regulating continuously learning AI systems presents unresolved questions for both developers and regulatory agencies seeking to ensure patient safety. Traditional medical device approval assumes that the approved product remains substantially unchanged throughout its commercial life, with any significant modifications requiring supplementary approval. AI systems that update their algorithms based on new clinical data fundamentally challenge this static approval paradigm, because the algorithm that receives regulatory clearance may differ substantially from the algorithm operating in clinics months or years later. Several regulatory frameworks for adaptive AI are under development at the FDA, European Medicines Agency, and other national regulatory bodies. These emerging frameworks attempt to define acceptable bounds for algorithm evolution while requiring manufacturers to demonstrate that algorithm updates maintain or improve performance relative to the originally approved version.
Where AI in Ophthalmology Is Heading Next
The trajectory of AI in ophthalmology points toward increasingly sophisticated applications that will reshape clinical practice, research methodology, and public health eye care delivery over the coming decade. Oculomics, the emerging field of using retinal imaging to detect systemic diseases beyond the eye, represents one of the most exciting frontiers in ophthalmic AI research. Deep learning models have demonstrated the ability to predict cardiovascular risk factors, Alzheimer’s disease biomarkers, and kidney function indicators from standard retinal photographs, suggesting that routine eye examinations could become windows into overall systemic health. If validated at scale, these capabilities would transform the role of ophthalmology from a specialty focused exclusively on eye disease to a screening gateway for multiple chronic conditions. The routine eye examination could become one of the most information-rich medical encounters in all of healthcare, with AI extracting insights about cardiovascular, neurological, and metabolic health from a single set of retinal images. The evolution of AI in drug discovery parallels the ophthalmic AI trajectory, as both fields leverage deep learning to extract hidden patterns from complex biological data.
Large language models are beginning to demonstrate specialist-level performance in answering ophthalmic clinical questions, suggesting that AI will soon augment not just imaging analysis but the full scope of clinical reasoning in eye care. GPT-4 and similar models have shown the ability to interpret clinical scenarios, recommend diagnostic workups, and suggest treatment plans with accuracy approaching that of practicing ophthalmologists in controlled testing scenarios. These conversational AI capabilities could support clinical decision-making by serving as always-available second opinions that help clinicians consider diagnoses and management strategies they might otherwise overlook. The integration of large language models with imaging analysis AI could create comprehensive clinical support systems that combine visual diagnostic capabilities with medical knowledge reasoning in a unified platform.
Foundation models trained on massive ophthalmic imaging datasets are emerging as versatile tools that can be adapted for multiple downstream clinical tasks without requiring separate training for each application. Rather than building individual AI systems for diabetic retinopathy, glaucoma, AMD, and each additional condition, foundation models provide a shared representational backbone that captures general ophthalmic imaging features applicable across diseases. Fine-tuning these models for specific clinical applications requires far less data and computational resources than training specialized models from scratch. This approach accelerates the development timeline for AI tools targeting rare eye diseases and uncommon presentations that lack the large training datasets available for common conditions. The efficiency of the foundation model approach is critical for expanding AI coverage beyond the handful of conditions where large labeled datasets currently exist to the full spectrum of ophthalmic pathology encountered in clinical practice.
Key Insights
- Around 1.1 billion people worldwide are affected by visual impairment, with AI-powered screening offering scalable solutions for early detection in underserved populations.
- AI-powered diagnostic tools achieved 87% to 96% sensitivity for diabetic retinopathy detection in clinical trials, with IDx-DR becoming the first FDA-approved autonomous AI diagnostic system in any field of medicine in 2018.
- Deep learning systems demonstrated area-under-the-curve values around 0.95 for glaucoma detection from fundus photographs and OCT, with AI algorithms outperforming human graders by identifying glaucoma in 88-90% of cases versus 79-81% for trained clinicians.
- A JAMA Ophthalmology study revealed that less than 5% of diabetic patients received AI-based retinal screening from 2019 to 2023 despite demonstrated accuracy, highlighting persistent adoption barriers.
- The global AI in ophthalmology market was valued at $314.64 million in 2025 with projections reaching $7.22 billion by 2035 at a CAGR of 36.8%.
- A survey of ophthalmologists found that 78% identified AI as the most transformative trend in their specialty, ranking it far above all other available technologies.
- The ALLY Adaptive Cataract Treatment System uses AI densitometry to adjust fragmentation patterns based on lens morphology in real time, reducing phaco energy and improving day-one surgical outcomes.
- The Society for Artificial Intelligence in Vision and Ophthalmology was established in May 2025 as the first global society dedicated to advancing AI integration in clinical eye care.
Artificial intelligence is reshaping ophthalmology across every dimension of clinical practice, from autonomous screening in primary care offices to real-time surgical guidance in operating rooms. The evidence base supporting AI diagnostic accuracy is robust, with multiple FDA-approved systems achieving sensitivity and specificity rates that match or exceed human specialist performance. The global market for ophthalmic AI is growing at rates exceeding 25% annually as clinical validation data accumulates and regulatory pathways become more established. The most significant challenge facing the field is not technical capability but adoption, as demonstrated by the striking gap between AI screening accuracy and real-world deployment rates for diabetic retinopathy detection. Addressing barriers including reimbursement uncertainty, workflow integration complexity, clinician trust, and algorithmic bias will determine how quickly AI delivers on its promise to prevent blindness in millions of people worldwide. The ethical imperative to expand eye care access through AI technology must be balanced against the responsibility to ensure that these systems perform equitably across all populations they serve.
| Factor | Traditional Eye Care | AI-Enhanced Eye Care |
|---|---|---|
| Diagnostic Accuracy | Dependent on individual clinician expertise and experience level, with inter-observer variability of 10-20% across graders | Consistent algorithmic performance achieving 87-96% sensitivity across validated conditions regardless of operator |
| Screening Access | Limited to facilities with trained ophthalmologists, concentrated in urban academic centers | Deployable in primary care offices, mobile clinics, and remote locations with minimal specialist infrastructure |
| Speed of Diagnosis | Requires specialist review appointments with wait times of weeks to months in many health systems | Delivers screening results in minutes at the point of care during routine medical visits |
| Cost per Screening | High per-unit cost driven by specialist time, dedicated examination equipment, and facility overhead | Lower marginal cost per screening that decreases further as systems process higher patient volumes |
| Population Coverage | Screens only patients who actively seek specialist appointments, missing high-risk populations | Enables systematic screening of entire diabetic populations through primary care integration |
| Bias and Equity | Subject to unconscious clinician biases but adaptable through individual clinical judgment | May contain systematic algorithmic biases from unrepresentative training data requiring active monitoring |
| Progression Monitoring | Relies on subjective comparison of serial images with significant measurement variability | Provides quantitative, reproducible measurements of disease change across imaging sessions |
Real-World Examples
IDx-DR Autonomous Diabetic Retinopathy Screening in Primary Care
The IDx-DR system, now LumineticsCore, demonstrated autonomous diabetic retinopathy detection across 900 patients at ten primary care sites throughout the United States in a pivotal clinical trial. The system achieved 87.2% sensitivity and 90.7% specificity for detecting more than mild diabetic retinopathy, leading to the first FDA authorization of an autonomous AI diagnostic system in any medical field in 2018. The trial showed an imageability rate of 96.1%, meaning the vast majority of patients produced usable images without the need for pupil dilation. The system enables primary care providers to offer specialist-level diabetic eye screening during routine diabetes management visits, eliminating the referral gap that causes many patients to miss annual eye examinations. A limitation of this deployment model is the less-than-5% adoption rate among diabetic patients nationally from 2019 to 2023, suggesting that FDA approval alone is insufficient to drive widespread clinical implementation without supporting reimbursement, education, and workflow integration initiatives.
Moorfields Eye Hospital and DeepMind AI for Retinal Disease
Moorfields Eye Hospital in London partnered with DeepMind Health to develop an AI system that analyzes OCT scans to detect and triage more than 50 retinal conditions, including diabetic eye disease, macular degeneration, and glaucoma, with accuracy matching leading retinal specialists as reported by research teams. The system was trained on a dataset of thousands of anonymized OCT scans from Moorfields patients, creating one of the most comprehensive retinal imaging AI models ever developed. The measurable outcome included referral accuracy that reduced unnecessary specialist appointments while ensuring that urgent cases received timely intervention. The partnership evolved into the formation of Cascader Limited in May 2025, a joint venture with Topcon Healthcare to commercialize AI-driven oculomics. A critique of this deployment centers on data governance concerns about the transfer of NHS patient data to a commercial technology company, with questions about consent, data ownership, and whether public health system data should benefit private sector entities.
AI Screening Programs in Rural India
Community-based AI screening programs in rural India have deployed portable retinal cameras with cloud-based AI analysis to screen diabetic populations in areas where no ophthalmologist is available within reasonable travel distance. The programs use smartphone-adapted fundus cameras operated by community health workers who receive brief training on image capture technique and patient positioning. Screening results are transmitted via mobile networks to cloud platforms that return AI analysis within minutes, enabling same-day triage decisions about which patients require referral to distant specialty centers. The measurable impact includes detection of vision-threatening diabetic retinopathy in patients who had never previously received eye examinations despite years of diabetes diagnosis. The growth of AI-driven medical screening in underserved regions demonstrates both the potential and limitations of these programs, as patients identified with treatable conditions still face significant barriers to accessing the surgical or injection-based treatments available only at distant specialty hospitals.
Case Studies
DHL of Diabetic Retinopathy Screening Through EyeArt at Federally Qualified Health Centers
Federally qualified health centers serving low-income and uninsured patients in the United States face a persistent challenge in meeting diabetic retinopathy screening guidelines because their patient populations often lack access to ophthalmology specialists. Several FQHCs implemented the EyeArt autonomous AI screening system to address this gap, deploying non-mydriatic retinal cameras in diabetes care clinics staffed by primary care providers. The EyeArt system demonstrated 96% sensitivity and 88% specificity for detecting more than mild diabetic retinopathy across diverse patient populations, and patients screened positive were immediately scheduled for ophthalmology referral through established specialty networks. The measurable impact included significant increases in screening rates among previously unscreened diabetic patients, with some sites reporting that AI screening enabled them to meet quality measures for diabetic eye examination compliance for the first time. A limitation is that the system cannot detect conditions outside its trained scope, meaning patients with non-diabetic retinal pathology or anterior segment disease identified only through comprehensive dilated examination may receive false reassurance from a negative AI screening result. The source for EyeArt performance data comes from published clinical trial results.
AI-Guided Cataract Surgery with the ALLY System
The integration of AI into laser cataract surgery through the ALLY Adaptive Cataract Treatment System represents a milestone in ophthalmic surgical technology that addresses long-standing sources of human error and variability. The system uses AI to analyze iris anatomical markers for precise registration without manual marking, and adjusts nuclear fragmentation patterns based on individual lens morphology and cataract density characteristics detected through AI densitometry. Surgeons using the ALLY system at multiple clinical sites reported reduced phaco energy delivery during procedures, which correlated with less corneal edema on postoperative day one and improved early visual outcomes. The measurable impact includes higher consistency in astigmatism correction accuracy across surgeons of varying experience levels, effectively democratizing access to precision surgical outcomes that were previously achievable only by the most experienced refractive surgeons. The controversy surrounding AI-assisted surgery involves concerns about deskilling, where surgeons who rely heavily on AI guidance may lose the ability to perform manual procedures effectively when technology fails or is unavailable. Performance data and clinical observations are detailed in presentations from Hawaiian Eye 2026.
Glaucoma Detection AI at Arvato and University College London
Researchers at University College London Institute of Ophthalmology and Moorfields Eye Hospital conducted a population-based cohort study comparing AI algorithm performance against experienced human graders for identifying glaucoma across 6,304 fundus images from diverse patient populations. The AI algorithm correctly identified patients with glaucoma in 88% to 90% of cases, significantly outperforming human graders who achieved 79% to 81% accuracy on the same image set. This performance gap demonstrated that AI systems can exceed human diagnostic accuracy for glaucoma detection when provided with standardized fundus photography inputs. The measurable impact includes the potential to implement population-scale glaucoma screening programs that do not require ophthalmologist involvement at the initial assessment stage, dramatically expanding screening capacity beyond what current specialist staffing levels can support. The limitation noted by researchers involves the reliance on curated imaging datasets that may not fully represent the range of image quality and patient demographics encountered in real-world mass screening campaigns. Results and methodological details are available through reporting by Ophthalmology Times.
Frequently Asked Questions
AI systems use deep learning algorithms trained on hundreds of thousands of labeled retinal images to recognize visual patterns associated with specific eye diseases. Convolutional neural networks process fundus photographs and OCT scans to identify features like microaneurysms, hemorrhages, drusen, and nerve fiber layer thinning. The algorithms classify images into disease categories and severity levels with accuracy matching or exceeding specialist performance.
AI diagnostic systems have demonstrated high accuracy for diabetic retinopathy, glaucoma, age-related macular degeneration, diabetic macular edema, and retinopathy of prematurity. Diabetic retinopathy screening tools achieve 87% to 96% sensitivity in clinical trials. Glaucoma detection algorithms achieve area-under-the-curve values around 0.95 using fundus photography. Research is expanding into cataracts, refractive errors, and rare retinal conditions.
Multiple AI-based ophthalmic diagnostic devices have received FDA authorization for clinical use in the United States. LumineticsCore, EyeArt, and devices from AEYE Health are among the approved autonomous screening systems for diabetic retinopathy. The European Union has its own regulatory framework governing AI medical devices, and approval pathways vary across other countries.
AI serves as a powerful screening and diagnostic support tool but does not replace the comprehensive clinical judgment of trained ophthalmologists. Autonomous AI systems can perform initial screening and triage in settings where ophthalmologists are unavailable. Complex clinical decisions involving treatment selection, surgical planning, and management of multiple concurrent conditions still require human specialist expertise and patient communication skills.
Costs vary depending on the healthcare system, insurance coverage, and specific device used. CPT code 92229 allows providers to bill for AI-based diabetic retinopathy screening in the United States, reducing out-of-pocket costs for insured patients. In many screening programs, AI assessment costs less per patient than traditional specialist evaluation. Some community health programs offer AI screening at no cost to patients as part of public health initiatives.
AI screening generates digital retinal images that contain biometric data potentially linkable to individual identities. Cloud-based AI platforms require images to be transmitted and processed on remote servers, raising questions about data security during transmission and storage. Patient consent processes must clearly explain how images will be used, stored, and potentially shared for algorithm development purposes.
AI enhances cataract surgery through improved preoperative planning, intraoperative guidance, and IOL power calculation accuracy. AI-driven systems analyze lens morphology and adjust surgical parameters in real time to optimize each procedure. Automated iris registration eliminates manual marking errors that can compromise astigmatism correction accuracy. AI-powered IOL calculation tools consider more variables than traditional formulas to predict postoperative refractive outcomes.
Oculomics uses retinal imaging data analyzed by AI to detect systemic health conditions beyond traditional eye diseases. Deep learning models can predict cardiovascular risk factors, neurological biomarkers, and metabolic indicators from standard retinal photographs. This field could transform routine eye examinations into comprehensive health screening encounters that provide information about multiple organ systems from a single noninvasive imaging session.
Current AI tools demonstrate strong overall performance but may show reduced accuracy for specific demographic subgroups underrepresented in training datasets. Models trained predominantly on patients of European descent may perform differently on patients with darker fundus pigmentation. Ensuring equitable performance requires diverse training datasets, validation across demographic groups, and ongoing monitoring for disparate outcomes in deployed systems.
Tele-ophthalmology combines portable imaging devices with cloud-based AI analysis to deliver screening in locations where patients cannot access ophthalmologists. Community health workers capture retinal images using portable cameras and receive AI analysis results within minutes. This model extends specialist-level screening to rural areas, developing countries, and underserved communities where traditional eye care infrastructure does not exist.
AI-based retinal screening typically adds only five to ten minutes to a primary care visit. Retinal image capture takes approximately two minutes per eye, and the AI system returns results within one to three minutes. Many systems work through undilated pupils, eliminating the thirty to forty minute wait required for pupil dilation in traditional examinations.
The Society for Artificial Intelligence in Vision and Ophthalmology was founded in May 2025 as the first global organization dedicated to ophthalmic AI. The American Academy of Ophthalmology has established AI task forces and published position statements on AI integration. Professional journals including Artificial Intelligence in Vision and Ophthalmology provide peer-reviewed venues for publishing ophthalmic AI research and clinical experience.
Medical education curricula are beginning to incorporate AI literacy, data science fundamentals, and critical evaluation skills for assessing AI diagnostic tools. Residents will need to understand algorithm development, validation methodology, and the appropriate clinical contexts for using AI-assisted diagnosis. AI-analyzed surgical video could transform how surgical skills are taught by providing objective performance metrics and personalized feedback.
The primary barriers include limited clinician awareness and trust in AI tools, inadequate reimbursement policies, challenges integrating AI systems with existing electronic health records, algorithmic bias concerns, and regulatory uncertainty for continuously learning systems. Cultural resistance among physicians who view AI as threatening to professional autonomy presents an adoption hurdle that technical performance alone cannot overcome.
AI models can predict disease progression risk by analyzing imaging features and clinical data that correlate with future vision loss trajectories. Sequence-aware models detect glaucoma visual field worsening up to 1.7 years earlier than conventional analysis methods. Predictive models for AMD and diabetic retinopathy identify patients at highest risk of rapid deterioration, enabling intensified monitoring and treatment before irreversible damage occurs.