
Introduction
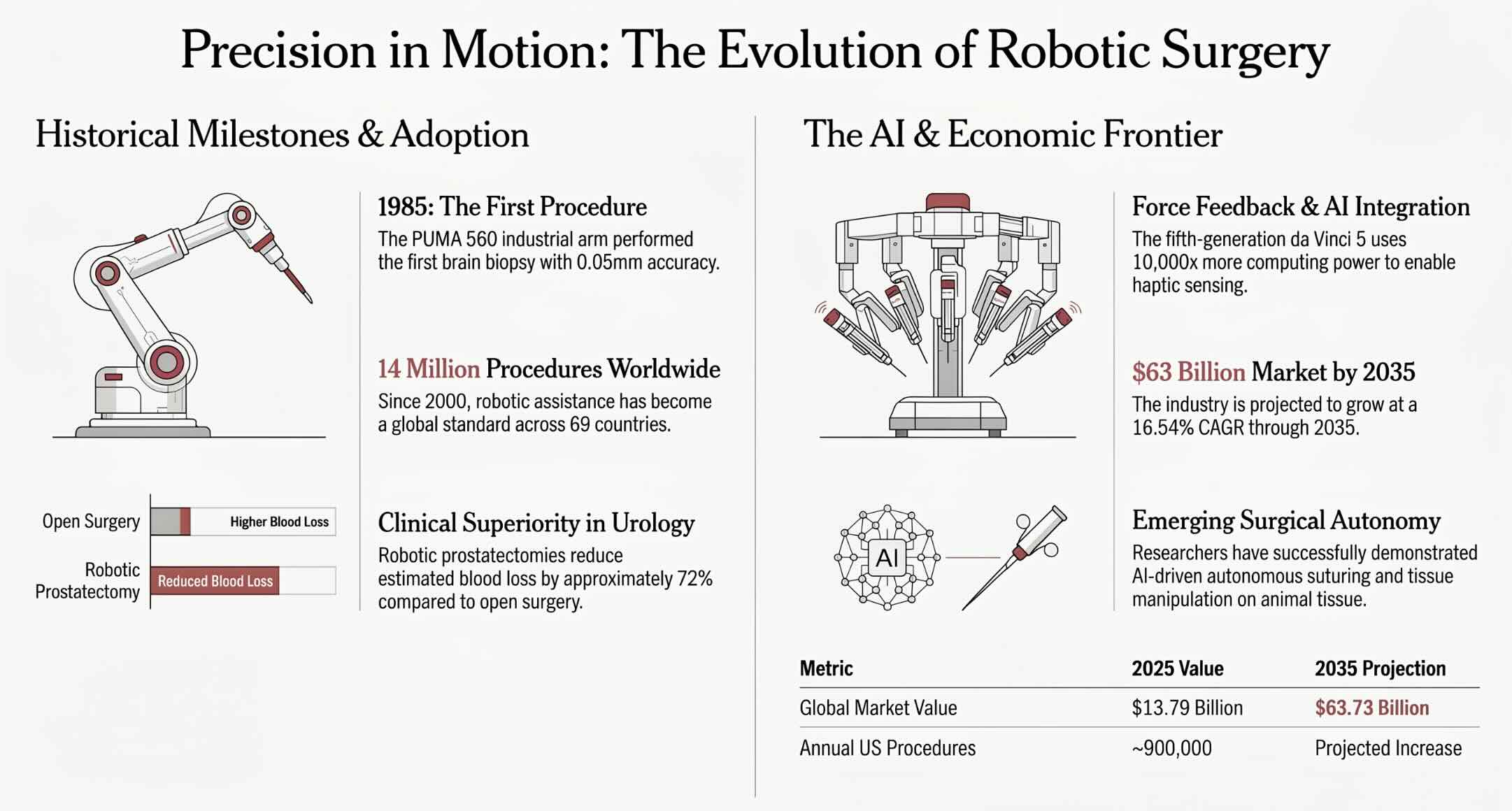
The operating room has undergone a quiet revolution that stretches back further than most patients and physicians realize. The first robotic surgery took place in 1985, when the PUMA 560 robotic arm assisted with a stereotactic brain biopsy at Memorial Medical Center in Long Beach, California. According to research published in the Journal of Endourology, this modified industrial robot inserted a needle into the brain with 0.05 millimeter accuracy, eliminating the hand tremors that plagued neurosurgeons during delicate biopsies. That single procedure launched a transformation that now encompasses over 14 million robotic-assisted surgeries performed worldwide and a global market valued at $13.79 billion in 2025. The journey from a repurposed factory arm to the fifth-generation da Vinci 5 platform with force feedback and AI integration tells the story of how technology reshapes medicine. Understanding when robotic surgery began reveals not just a historical timeline but the forces that continue to push surgical innovation forward. The 1985 brain biopsy using the PUMA 560 marked the birth of a field that now defines modern surgical care across every major medical specialty.
Quick Answers About the First Robotic Surgery
Which robot performed the first robotic surgery?
ROBODOC performed the first robotic-assisted hip replacement on November 7, 1992, at Sutter General Hospital in Sacramento, California, on a 64-year-old patient with osteoarthritis.
What was the firs robotic surgery?
The first robotic surgery was performed in 1985 using the PUMA 560 robotic arm for a CT-guided stereotactic brain biopsy, achieving precision that exceeded human hand capabilities.
What was thee first FDA-cleared robotic surgical system?
The first FDA-cleared robotic surgical system for active surgery was the da Vinci Surgical System, approved in July 2000 for general laparoscopic procedures by Intuitive Surgical.
Key Takeaways
- The global robotic surgery market is projected to grow from $13.79 billion in 2025 to over $63 billion by 2035, driven by AI integration, new competitors, and expanding surgical applications.
- The PUMA 560 performed the first robotic surgery in 1985, a brain biopsy that demonstrated robotic precision could surpass human steadiness in neurosurgical procedures.
- ROBODOC completed the first robotic hip replacement in 1992, and its prototype is now preserved in the Smithsonian Institution as a landmark medical innovation.
- The da Vinci Surgical System received FDA clearance in 2000 and has since facilitated over 14 million procedures across more than 7,500 installed systems worldwide.
Table of contents
- Introduction
- Quick Answers About the First Robotic Surgery
- Key Takeaways
- Defining Robotic Surgery
- The 1985 Brain Biopsy That Started It All
- PROBOT and the Expansion Into Urology
- ROBODOC and the First Robotic Hip Replacement
- Military Origins: DARPA, NASA, and Telesurgery
- Computer Motion, AESOP, and the ZEUS System
- The da Vinci Surgical System: Transforming Modern Surgery
- Evolution Across Five Generations of da Vinci
- Da Vinci 5: Force Feedback and AI Integration
- The Rise of Competition: Hugo, Versius, and Beyond
- Clinical Outcomes: What the Evidence Shows
- Cost Considerations and Hospital Economics
- Robotic Surgery Across Medical Specialties
- The Surgeon Training Challenge
- AI and the Path Toward Surgical Autonomy
- Ethical Questions in Robotic and Autonomous Surgery
- Global Adoption and Emerging Markets
- What Patients Should Know About Robotic Surgery Today
- The Future of Robotic Surgery: 2026 and Beyond
- Key Insights
- Milestones in Robotic Surgery Evolution
- Real-World Examples
- Case Studies
- Frequently Asked Questions About the First Robotic Surgery
Defining Robotic Surgery
Robotic surgery is a minimally invasive surgical approach in which a surgeon controls robotic instruments from a console, using computer-enhanced technology to translate hand movements into precise actions of miniaturized tools inside the patient’s body, improving visualization, dexterity, and accuracy beyond unaided human capabilities.
Robotic Surgery Explorer
Explore the history, clinical outcomes, and market growth of robotic surgery from 1985 to today.
The global robotic surgery market is projected to grow from $13.79 billion in 2025 to over $63 billion by 2035, driven by new competitors, AI integration, and expansion into more specialties.
The 1985 Brain Biopsy That Started It All
The PUMA 560 was never designed for the operating room. Manufactured by Unimation for industrial assembly lines, this robotic arm found its way into surgical history when researchers recognized its potential for eliminating the hand tremors that introduced dangerous imprecision during neurosurgical needle placement. Computed tomography guided the robot as it inserted a biopsy needle into the brain with sub-millimeter accuracy, achieving a level of precision that the steadiest human hand could not match. The procedure took place at a time when the word "robot" in medicine sounded more like science fiction than clinical reality. Programmable Universal Machine for Assembly, the full name behind PUMA, reflected its factory-floor origins rather than any medical ambition. The 1985 brain biopsy using the PUMA 560 is universally recognized as the first robotic surgery in medical history, transforming an industrial tool into a surgical pioneer.
The success of the PUMA 560 demonstrated two principles that would drive the next four decades of robotic surgical development. Robots could eliminate unwanted motion, and they could position instruments with a repeatability that human anatomy simply cannot achieve. These findings inspired researchers across multiple surgical specialties to explore how robotic assistance might improve outcomes in their own fields. The PUMA 560 biopsy did not replace the neurosurgeon; it augmented the surgeon's capabilities in a way that reduced risk for the patient. This distinction between replacement and augmentation would become central to how the entire field of AI in robotics evolved over subsequent decades.
PROBOT and the Expansion Into Urology
Three years after the PUMA 560 brain biopsy, researchers at Imperial College London adapted the same robotic platform for an entirely different surgical challenge. In 1988, Brian Davies and his team used a modified version of the PUMA system to perform a transurethral resection of the prostate, a procedure that required numerous repetitive cutting motions with consistent depth and angle. The modified system became known as PROBOT, the first robotic platform specifically designed for a urological surgical application. Where the PUMA 560 brain biopsy demonstrated precision in a single needle placement, PROBOT showed that robots could handle the repetitive, fatigue-inducing motions that cause surgeons to lose consistency over the course of lengthy procedures. PROBOT represented a critical conceptual leap: robotic surgery was not limited to one-time precision tasks but could enhance entire procedural workflows requiring sustained accuracy.
The transition from neurosurgery to urology proved that robotic assistance had applications far beyond the brain. Prostate surgery demanded a different set of capabilities, including the ability to make consistent cuts across tissue while preserving surrounding structures. PROBOT's success at Imperial College London encouraged other research groups to begin developing specialty-specific robotic systems rather than trying to adapt a single industrial robot to every surgical context. This specialization would accelerate the development of healthcare automation tools tailored to the unique demands of different surgical disciplines, setting the stage for the orthopedic revolution that followed.
ROBODOC and the First Robotic Hip Replacement
The story of ROBODOC begins with an unlikely partnership between an orthopedic surgeon and a veterinarian in Sacramento, California. Dr. William Bargar, an orthopedic surgeon at Sutter Medical Center, and his colleague Hap Paul, a doctor of veterinary medicine, recognized that the precision required for preparing the femoral cavity during hip replacement surgery exceeded what surgeons could consistently achieve by hand. They developed ROBODOC through Integrated Surgical Systems in collaboration with IBM, creating the first robotic system capable of actively milling bone during a surgical procedure. On November 7, 1992, ROBODOC performed its first human hip replacement at Sutter General Hospital on a 64-year-old man struggling with osteoarthritis. The surgery was successful, and news outlets described a seven-foot robot with steadier hands than any human surgeon. ROBODOC's 1992 hip replacement was the first robotic surgery involving active bone cutting, and its prototype now resides in the Smithsonian Institution as a testament to surgical innovation.
Ten additional robot-assisted hip replacements followed under an investigational device exemption approved by the FDA on October 9, 1992. ROBODOC allowed surgeons to pre-plan their operations using CT imaging and then execute those plans with a precision that manual techniques could not replicate. The system optimized prosthesis sizing on a patient-specific basis, addressing a long-standing challenge in joint replacement surgery where imprecise cavity preparation led to poor implant fit and premature failure. ROBODOC gained acceptance across Europe, where thousands of procedures were performed, though it initially did not receive FDA marketing clearance in the United States due to concerns about complication rates. THINK Surgical Inc. eventually acquired the technology and found the historic prototype in a storage unit, donating it to the Smithsonian's medical and science division for permanent preservation.
Military Origins: DARPA, NASA, and Telesurgery
The technological foundations of modern robotic surgery extend beyond the hospital into the corridors of military research laboratories and space agencies. The Defense Advanced Research Projects Agency (DARPA) funded research into telemanipulation systems in the late 1980s and early 1990s with a specific military objective: enabling surgeons to operate on wounded soldiers from a safe distance behind the front lines. Stanford Research Institute developed a system of robotic telemanipulation for microsurgery under contract to the military, while NASA explored similar technologies for performing surgery on astronauts during long-duration space missions. These parallel tracks of military and space research produced the master-slave concept, where a surgeon's hand movements at a console are transmitted to robotic instruments at the patient's side. The modern surgical robot owes its fundamental architecture to Cold War-era military research and NASA's ambition to deliver medical care in the most remote environments imaginable.
The virtual reality pioneer Scott Fisher developed the first head-mounted display at NASA, immersing the viewer in a three-dimensional environment that became a precursor to the 3D visualization systems used in today's surgical consoles. Engineer Phil Green at Stanford Research Institute created telemanipulation prototypes that demonstrated how a surgeon's movements could be faithfully reproduced by robotic instruments at a distance. These technologies merged the concepts of telepresence and robotic manipulation into a unified surgical platform. The impact of artificial intelligence in healthcare can be traced directly to these government-funded research programs that translated military requirements into civilian medical breakthroughs.
Computer Motion, AESOP, and the ZEUS System
The first commercial company dedicated entirely to surgical robotics was Computer Motion, founded in August 1989 by Yulun Wang with the explicit goal of revolutionizing surgical practice. The company's initial product was AESOP (Automated Endoscopic System for Optimal Positioning), a voice-controlled robotic arm that held and positioned an endoscopic camera during laparoscopic surgery. AESOP solved a persistent problem: laparoscopic surgeons relied on human assistants to hold the camera steady, but assistants fatigued, shifted position, and could not respond instantaneously to verbal commands the way a robot could. AESOP received FDA clearance in 1994, making it the first robotic device cleared for use in an operating room in the United States. Computer Motion then developed the ZEUS Robotic Surgical System, a more ambitious platform that gave surgeons telemanipulation control over multiple instruments. AESOP's 1994 FDA clearance marked the moment when robotic surgical devices moved from research prototypes into commercially available clinical tools.
The ZEUS system gained regulatory approval in Europe and was used for a landmark achievement in September 2001, when surgeon Jacques Marescaux in New York performed a cholecystectomy on a patient in Strasbourg, France, using ZEUS over a dedicated fiber-optic connection. This "Operation Lindbergh" demonstrated that telesurgery across thousands of miles was technically feasible, though latency issues and the need for dedicated high-speed connections limited its practical application. Computer Motion and Intuitive Surgical, the company behind the rival da Vinci system, became locked in patent litigation that hindered both companies' growth. The dispute was resolved in 2003 when Intuitive Surgical acquired Computer Motion in a merger, and the ZEUS system was phased out in favor of the da Vinci platform that would come to dominate robotic surgical innovation.
The da Vinci Surgical System: Transforming Modern Surgery
Intuitive Surgical was founded in 1995 by Frederick Moll and Robert Younge, who developed a prototype robotic surgical system nicknamed "Lenny" that evolved through iterations called "Leonardo" and "Mona" before the final version received the name da Vinci. The name honored Leonardo da Vinci's study of human anatomy, which eventually led to the design of the first known robot in history. After testing in Europe beginning in 1999, the da Vinci Surgical System received FDA clearance on July 11, 2000, for general laparoscopic surgery. FDA Commissioner Jane Henney described the approval as the first step in robotic technology that could change the practice of surgery. The system combined a surgeon's console with a patient-side cart carrying robotic arms, a high-definition 3D vision system, and proprietary EndoWrist instruments that could bend and rotate with greater range than the human hand. The da Vinci system's July 2000 FDA approval established artificial intelligence in healthcare as a commercially viable platform and launched the era of widespread robotic-assisted minimally invasive surgery.
Surgeons in Belgium had used an early version of the system in 1997 for robotic cholecystectomy and Nissen fundoplication, demonstrating the platform's versatility across different procedure types. The FDA expanded approvals to include prostate surgery in 2001, thoracoscopic procedures, cardiac surgery in 2002, and gynecologic procedures in subsequent years. By 2012, the da Vinci system was used in approximately 200,000 surgeries annually, with prostatectomy and hysterectomy accounting for over 70 percent of robotic procedures. The system's three-dimensional magnification screen provided surgeons with visualization clarity that exceeded traditional laparoscopic cameras, while the one-centimeter diameter surgical arms represented a dramatic miniaturization from the large industrial arms of earlier systems like the PUMA 560.
Evolution Across Five Generations of da Vinci
The da Vinci platform has progressed through five distinct generations, each addressing limitations discovered in clinical practice. The original system established the basic architecture of surgeon console, patient cart, and vision system. In 2003, a fourth robotic arm was added, giving surgeons greater instrument flexibility during complex procedures. The da Vinci S model arrived in 2006 with improved arm movements, enhanced console displays, and simpler setup procedures. The da Vinci Si launched in 2009, introducing dual consoles that allowed two surgeons to collaborate simultaneously during a procedure. The da Vinci Xi, which remains the workhorse multiport system at thousands of hospitals, featured overhead-mounted arms that could rotate around the patient for access to multiple surgical quadrants without repositioning. Each generation of the da Vinci system reflected specific feedback from thousands of surgeons performing tens of thousands of procedures, creating an iterative improvement cycle unprecedented in surgical device history.
The da Vinci SP (Single Port), designed for procedures requiring access through a single small incision or natural orifice, demonstrated the platform's ability to address specialized surgical needs beyond general multiport applications. The da Vinci X provided a value-oriented entry point for hospitals beginning their robotic surgery programs, built on the same arm architecture as the Xi but with a lower acquisition cost. These platform variants allowed Intuitive Surgical to serve different hospital sizes, budgets, and surgical volumes, expanding robotic surgery from elite academic medical centers into community hospitals and ambulatory surgical centers.
Da Vinci 5: Force Feedback and AI Integration
The fifth generation da Vinci 5 represents the most significant technological leap in the platform's history. Redesigned with over 150 design innovations and 10,000 times the computing power of the da Vinci Xi, the system introduces force feedback technology for the first time in the da Vinci product line. Surgeons can now sense the push and pull forces at the instrument tip, a capability that previous generations entirely lacked. Early preclinical data indicates that surgeons with varying experience levels delivered up to 43 percent less force on tissue when using force feedback instruments, potentially reducing tissue trauma and improving patient recovery outcomes. The system features a unified control interface that allows surgeons to manage insufflation, imaging, cautery energy, and audio settings from the console without relying on team members to adjust equipment manually. The da Vinci 5's introduction of haptic feedback and AI-powered analytics transforms the surgical robot from a passive instrument translator into an active partner in surgical decision-making.
Cloud connectivity enables the da Vinci 5 to gather and process surgical data globally, creating opportunities for video replay, digital case analysis, performance metrics, and personalized coaching. The system can track every movement a surgeon makes, developing algorithms that highlight differences between expert and novice techniques. This data-driven approach helps surgeons identify specific skills requiring improvement, moving surgical training from subjective mentorship toward objective, measurable performance development. Intuitive Surgical's CEO has described the system's strengths in motion control, advanced imaging, and AI integration as capabilities that could expand robotic surgery into cardiac procedures, an area where the company received FDA clearance for nine new indications in 2025.
The Rise of Competition: Hugo, Versius, and Beyond
Intuitive Surgical's near-monopoly in robotic surgery is facing meaningful competitive pressure for the first time in two decades. Medtronic developed the Hugo RAS (Robot-Assisted Surgery) system with a key innovation: a modular design featuring four independent robotic arms on separate carts, allowing surgeons to use only the arms needed for each specific procedure. British-based CMR Surgical achieved unicorn status with a $3 billion valuation in 2021 for its Versius system, which launched in 2019 and has completed over 20,000 procedures across 20 NHS hospitals and multiple countries. Versius's compact size and significantly lower cost, estimated at $1 to $1.5 million compared to the da Vinci's $2 to $2.5 million price tag, make it accessible to smaller operating theaters and hospitals in developing economies. Johnson and Johnson submitted an FDA de novo request for its OTTAVA Robotic Surgical System in January 2026, with early clinical cases for gastric bypass surgery already completed. The emergence of credible competitors to the da Vinci system is expected to drive down acquisition costs, expand access to robotic healthcare technology, and accelerate innovation across the entire surgical robotics industry.
India's indigenous surgical robotic system, SSI Mantra, made history in January 2025 by performing two world-first telesurgeries over a distance of 286 kilometers with a latency of only 40 milliseconds. SSI Mantra is currently the only approved product worldwide for telesurgery and teleproctoring, demonstrating that surgical robotics innovation is no longer confined to Silicon Valley and Western Europe. The Senhance system from TransEnterix (later Asensus Surgical) was a pioneer in haptic feedback and eye-tracking camera control, though the company faced financial difficulties and was acquired by Karl Storz in 2024. This competitive landscape represents the maturation of an industry that for years was essentially a single-company market.
Clinical Outcomes: What the Evidence Shows
The clinical evidence base for robotic surgery now encompasses over 38,000 peer-reviewed articles analyzing outcomes across virtually every surgical specialty. Robotic-assisted radical prostatectomy reduces mean estimated blood loss by approximately 72 percent compared to open surgery, a difference that translates directly into fewer transfusions and faster postoperative recovery. Patients undergoing robotic hysterectomy experience a 50 percent reduction in surgical site infection risk compared to open procedures. Robotic colorectal surgery is associated with a 1.5-day reduction in hospital length of stay, while the conversion rate from robotic to open surgery in gynecologic procedures remains below 5 percent in high-volume centers. These findings demonstrate measurable patient benefits across multiple procedure types. The accumulated evidence from 14 million procedures and 38,000 published studies has moved robotic surgery from experimental novelty to evidence-based standard of care in multiple surgical specialties.
The data on robotic surgery is not uniformly positive, and honest assessment requires acknowledging the limitations and controversies in the literature. Critics note that many comparative studies suffer from selection bias, as surgeons tend to choose robotic approaches for patients with favorable anatomy. Long-term outcome data showing clear superiority over well-performed laparoscopic surgery remains limited in several procedure categories. The steep learning curve associated with robotic systems means that outcomes vary substantially between novice and experienced robotic surgeons, introducing a variable that traditional surgical technique does not impose to the same degree. Thirty-day readmission rates for robotic partial nephrectomy are notably lower at approximately 3 percent, but whether this reflects the technology or the surgeons who self-select into robotic programs remains debated.
Cost Considerations and Hospital Economics
The economics of robotic surgery present a complex picture that goes beyond the headline acquisition price of the surgical system itself. A da Vinci system costs between $1.5 million and $2.5 million for the initial purchase, with annual maintenance contracts running $80,000 to $170,000 and disposable instruments consuming approximately $1,800 to $4,600 per procedure. These costs place robotic surgery systems beyond the reach of many community hospitals and healthcare facilities in developing countries. Instruments and accessories already account for over half of total market revenue, creating a recurring revenue model that benefits manufacturers but raises concerns about the total cost of ownership for hospitals. The financial calculus must weigh these costs against the documented benefits of shorter hospital stays, fewer complications, and reduced readmission rates. The tension between the high cost of robotic surgical systems and their demonstrated clinical benefits defines the economic debate around surgical robotics adoption in healthcare systems worldwide.
Intuitive Surgical's expiring patents are enabling new competitors to enter the field, and market analysts expect this competitive pressure to drive down system costs over the next five years. Leasing models already represent about 40 percent of new system placements, reducing the upfront capital burden for hospitals. Subscription and pay-per-use commercial models from newer competitors like CMR Surgical further lower the barrier to entry. The global robotic surgery market, valued at $13.79 billion in 2025, is projected to reach $63.73 billion by 2035, growing at a compound annual growth rate of 16.54 percent, suggesting that the economics will continue to improve as scale increases and competition intensifies.
Robotic Surgery Across Medical Specialties
Robotic surgical platforms have expanded from their origins in neurosurgery and orthopedics to encompass virtually every major surgical specialty. Urology led the adoption wave, with robotic-assisted radical prostatectomy becoming the dominant approach for prostate cancer surgery in the United States. Gynecology followed closely, with robotic hysterectomy becoming the most common robotic procedure alongside prostatectomy, together accounting for over 70 percent of all da Vinci procedures by 2010. General surgery applications expanded rapidly, with robotic techniques applied to hernia repair, cholecystectomy, bariatric surgery, and colorectal procedures. General surgery became the fastest-growing specialty for robotic adoption in the United States by 2021. The versatility of robotic surgical platforms across urology, gynecology, general surgery, cardiac surgery, and thoracic procedures demonstrates that the technology's benefits are not limited to a single medical application but represent a fundamental improvement in surgical capabilities.
Cardiac surgery represents the newest frontier for robotic expansion, with Intuitive Surgical receiving FDA clearance for nine new cardiac indications in 2025, including mitral and tricuspid valve repair, mitral valve replacement, and left atrial appendage closure. Robotic-assisted mitral valve repair demonstrates a zero percent sternotomy rate compared to 100 percent in conventional open heart surgery, a dramatic difference that translates into significantly reduced recovery times and surgical trauma. Orthopedic surgery continues to grow as one of the largest application areas, driven by rising joint replacement volumes and the increasing use of robotic systems that enhance surgical accuracy in knee and hip operations. Thoracic, head and neck, and neurosurgical applications continue to evolve as instrument miniaturization and platform flexibility improve.
The Surgeon Training Challenge
The introduction of robotic surgical systems has created a training challenge that the medical education system continues to address. Learning to operate a robotic console requires different skills than traditional open or laparoscopic surgery, and the transition involves a documented learning curve during which complication rates may be higher than for experienced surgeons. Studies show that surgeon proficiency with robotic systems typically requires 20 to 50 supervised cases, depending on the procedure complexity and the surgeon's prior laparoscopic experience. By 2018, approximately 35.1 percent of surgeons in the United States were performing robotic surgeries, up from 8.7 percent in 2012, indicating rapid but incomplete adoption of robotic skills across the surgical workforce. The da Vinci 5's data analytics capabilities offer a new approach to training, using objective performance metrics rather than subjective assessments. The shift from apprenticeship-based surgical training to data-driven performance analytics represents one of the most significant secondary effects of robotic technology in medicine.
Simulation-based training has become integral to robotic surgical education, allowing surgeons to practice procedures on virtual patients before operating on real ones. Dual-console systems, available since the da Vinci Si in 2009, enable experienced surgeons to guide trainees in real time during actual procedures, sharing control of the instruments and providing immediate feedback. Remote telepresence training, where expert surgeons observe and coach remotely, has expanded access to high-quality robotic surgical education beyond the major academic centers where expertise was historically concentrated. These educational innovations address the challenge of scaling robotic surgical skills to meet the growing demand for robotic procedures across community hospitals and emerging markets.
AI and the Path Toward Surgical Autonomy
Artificial intelligence is reshaping robotic surgery from a telemanipulation tool into a platform with increasing cognitive capabilities. Researchers at Johns Hopkins and Stanford Universities demonstrated in late 2024 that a vision-language model trained on 20 hours of surgical video could enable a da Vinci robot to autonomously perform key surgical tasks, including lifting tissue, manipulating needles, and suturing wounds on animal tissue. The AI system used imitation learning rather than detailed programming, observing what surgeons did in videos and reproducing those actions in novel environments. The retrofitted da Vinci robots even demonstrated problem-solving abilities, such as picking up a dropped surgical needle, that were not explicitly programmed. These experiments offer a glimpse into a future where certain surgical tasks might be performed autonomously, though experts emphasize that fully autonomous robotic surgery on human patients remains years away. AI integration in robotic surgery is moving beyond passive assistance toward active surgical intelligence, where machine learning models guide robotic actions in real time based on analysis of thousands of prior procedures.
Current AI applications in robotic surgery focus on decision support rather than autonomous operation. Real-time video analysis can identify anatomical structures and alert surgeons to critical landmarks during procedures. Predictive analytics assess tissue characteristics and suggest optimal approaches based on patient-specific anatomy. Companies like Anaut have received regulatory approval for software devices that use AI to analyze real-time video from laparoscopic and robotic surgery, enhancing the surgeon's accuracy without replacing their judgment. The da Vinci 5's 10,000-fold increase in computing power over previous generations positions it as a platform for deploying increasingly sophisticated AI tools. Experts at the Antal Bejczy Center for Intelligent Robotics note that billions of dollars have been invested in robotic surgery, but fully autonomous surgical robots remain a distant prospect given the ethical, legal, and technical challenges involved.
Ethical Questions in Robotic and Autonomous Surgery
The evolution of robotic surgery from simple telemanipulation toward AI-assisted decision-making raises ethical questions that the medical community must address proactively. The distinction between a robot that faithfully executes a surgeon's commands and one that suggests or initiates actions based on its own analysis represents a fundamental shift in the locus of surgical responsibility. If an AI system recommends an approach that leads to a complication, the allocation of liability between the surgeon, the hospital, and the technology manufacturer becomes legally complex. Patient consent must evolve to reflect the increasing role of AI in surgical decision-making, ensuring that patients understand not just the procedure but the degree to which algorithmic systems influence the surgical approach. The ethical dimensions of AI in surgery require updated governance frameworks that address accountability, transparency, and informed consent in ways that existing medical malpractice law was not designed to handle.
Data privacy presents additional ethical challenges as cloud-connected robotic systems collect and transmit detailed surgical performance data. Every movement a surgeon makes on the da Vinci 5 can be recorded, analyzed, and compared against performance benchmarks. While this data enables quality improvement and personalized training, it also creates surveillance concerns that could affect surgeon behavior and increase defensive medicine. Access equity is another ethical imperative: robotic surgery is overwhelmingly concentrated in wealthy nations and well-funded hospitals, creating a two-tier surgical system where patients in resource-limited settings lack access to technologies that demonstrably improve outcomes. Addressing this disparity through lower-cost systems, training programs, and telesurgery capabilities is as much an ethical obligation as a market opportunity.
Global Adoption and Emerging Markets
The geographic distribution of robotic surgery reveals stark disparities in access that mirror broader patterns of healthcare inequality. North America commands approximately 51 percent of the global surgical robotics market, driven by advanced healthcare infrastructure, high adoption rates, and the presence of leading manufacturers including Intuitive Surgical. As of 2023, over 7,500 da Vinci systems were installed in hospitals across 69 countries, but the concentration remains heavily skewed toward the United States, Europe, and affluent Asian nations like Japan and South Korea. China's installed base is growing rapidly, with the country representing one of the fastest-growing markets for robotic surgery systems. India's development of the indigenous SSI Mantra system reflects a growing recognition that dependence on imported robotic systems limits access and affordability. The Asia-Pacific region is projected to experience the fastest growth in robotic surgery adoption through 2035, driven by rising healthcare investment, expanding surgeon training programs, and the introduction of lower-cost alternatives to the da Vinci platform.
Telesurgery offers the most promising path to extending robotic surgical capabilities to underserved regions. SSI Mantra's successful telesurgeries across 286 kilometers in India demonstrate that latency challenges can be overcome with current network technology. The expansion of 5G networks in developing economies could enable remote surgical mentoring and eventually remote robotic surgery, allowing expert surgeons in major urban centers to guide or perform procedures at rural hospitals thousands of miles away. The entry of lower-cost competitors like Versius and Hugo RAS is also expanding the addressable market by making robotic systems financially viable for mid-sized hospitals and ambulatory surgical centers that could never justify the $2 million investment required for a da Vinci system.
What Patients Should Know About Robotic Surgery Today
Patients considering robotic surgery in 2026 benefit from nearly 900,000 robotic procedures performed annually in the United States alone and a wealth of clinical evidence supporting its use across major surgical specialties. The most important factor in robotic surgical outcomes is not the robot itself but the experience of the surgeon operating the system. High-volume surgeons at high-volume centers consistently achieve better outcomes than low-volume operators, and patients should ask about their surgeon's specific robotic experience, including the number of procedures performed and the complication rates observed. Recovery from robotic surgery is typically faster than from open surgery, with most patients returning to normal activities within two to three weeks. The conversion rate from robotic to open surgery is relatively low, ranging from 0.8 to 5 percent depending on the procedure and surgeon experience. Patients should approach robotic surgery as a tool that enhances their surgeon's capabilities rather than a guarantee of superior outcomes, and should prioritize surgeon experience and hospital volume above the presence of the technology itself.
The cost of robotic surgery to individual patients varies significantly based on insurance coverage, geographic location, and the specific procedure. In general, robotic procedures may carry higher facility charges than laparoscopic alternatives due to the capital and consumable costs associated with the robotic system. Insurance coverage for robotic surgery has expanded substantially as the evidence base has grown, and most major insurers now cover robotic-assisted procedures without distinguishing them from other minimally invasive approaches. Patients should discuss the specific advantages and limitations of robotic versus laparoscopic or open approaches for their particular condition, as not every surgery benefits equally from robotic assistance.
The Future of Robotic Surgery: 2026 and Beyond
The robotic surgery landscape in 2026 and beyond is defined by the convergence of multiple technological trends that promise to expand both the capabilities and accessibility of robotic-assisted procedures. AI-powered real-time surgical guidance, micro-robotics that can perform targeted tasks inside the body, augmented reality overlays that project patient anatomy onto the surgical field, and fully autonomous suturing capabilities are all advancing from laboratory demonstrations toward clinical applications. Intuitive Surgical forecasts worldwide da Vinci procedure growth of 13 to 15 percent in 2026, while the competitive entry of systems from Medtronic, Johnson and Johnson, CMR Surgical, and other manufacturers is expected to accelerate market expansion beyond what a single-vendor ecosystem could achieve. The global surgical robotics market is projected to exceed $50 billion by 2035, reflecting both the growing volume of robotic procedures and the expanding range of surgical applications. The next decade of robotic surgery will be defined not by a single dominant platform but by a competitive ecosystem where AI integration, lower costs, and expanded access transform surgical care across every region and economic tier worldwide.
The longer-term vision includes micro-sized surgical robots guided by external magnets that can navigate inside the body to perform targeted interventions, eliminating the need for even the small incisions required by current robotic laparoscopic approaches. Digital twin technology, where a virtual replica of the patient's anatomy is created from imaging data and used to simulate the procedure before it begins, is already being integrated into surgical planning workflows. Haptic internet technology could enable telesurgery across global distances with latency low enough to make real-time robotic surgical control indistinguishable from bedside operation. These advances collectively point toward a future where the geographic limitations and access barriers that currently define surgical care are progressively dismantled through robotic and AI-enabled technologies.
Key Insights
- The PUMA 560 performed the first robotic surgery in 1985 for a stereotactic brain biopsy, achieving 0.05 millimeter accuracy that exceeded the steadiest human hand, establishing the foundational principle that robotic precision could enhance surgical outcomes.
- Over 14 million robotic-assisted procedures have been performed worldwide as of 2025, with da Vinci systems installed in more than 7,500 hospitals across 69 countries, making robotic surgery one of the most widely adopted medical technologies of the 21st century.
- The global robotic surgery market was valued at $13.79 billion in 2025 and is projected to reach over $63 billion by 2035, growing at a CAGR of 16.54 percent driven by AI integration, competitive market entry, and expanding surgical applications.
- Robotic-assisted radical prostatectomy reduces estimated blood loss by approximately 72 percent compared to open surgery, while robotic hysterectomy cuts surgical site infection risk by 50 percent, demonstrating measurable clinical superiority in key procedure categories.
- Intuitive Surgical's revenue grew from $1.41 billion in 2010 to over $10 billion in 2025, reflecting the commercial scale of robotic surgery adoption and the company's dominant 70 to 80 percent global market share.
- The da Vinci 5 system features 10,000 times the computing power of the da Vinci Xi, introduces force feedback for the first time in the platform's history, and enables AI-powered surgical analytics and personalized surgeon coaching.
- Researchers at Johns Hopkins and Stanford demonstrated that a vision-language model trained on 20 hours of surgical video could enable a da Vinci robot to autonomously perform key surgical tasks on animal tissue, foreshadowing the path toward surgical AI autonomy.
- India's SSI Mantra system performed the first telesurgeries over 286 kilometers with 40-millisecond latency in January 2025, demonstrating that remote robotic surgery is technically viable for extending surgical expertise to underserved regions.
The first robotic surgery in 1985 launched a trajectory that has reshaped surgical care across every major medical specialty and geographic region. From the PUMA 560's brain biopsy through ROBODOC's orthopedic milestone and the da Vinci system's commercial dominance, each generation of robotic surgery has expanded what is surgically possible while reducing patient trauma and recovery times. The accumulated evidence from over 14 million procedures and 38,000 published studies supports robotic surgery's role as a standard of care in urology, gynecology, and general surgery. Market projections exceeding $50 billion by 2035 reflect genuine clinical adoption rather than speculative investment. The integration of AI, force feedback, and cloud analytics in the da Vinci 5 signals a new phase where robotic surgery becomes intelligent rather than merely precise. What remains to be determined is whether the competitive entry of lower-cost systems and the expansion of telesurgery can close the global access gap that currently limits robotic surgical care to the world's wealthiest healthcare systems.
Milestones in Robotic Surgery Evolution
| Dimension | Early Era (1985-1999) | Growth Era (2000-2019) | Modern Era (2020-2026) |
|---|---|---|---|
| Transparency | Research prototypes; limited published outcomes; experimental device exemptions | Growing evidence base; thousands of peer-reviewed studies; FDA clearance pathways established | Over 38,000 published articles; cloud-connected data analytics; AI-powered performance tracking |
| Participation | Confined to academic research centers; fewer than 10 systems worldwide; specialist surgeons only | Rapid hospital adoption; thousands of installations; training fellowships expand access | Over 7,500 systems in 69 countries; multiple competing platforms; telesurgery extends reach |
| Trust | Skepticism from surgical establishment; unproven technology; limited clinical evidence | Growing acceptance; professional society endorsements; patient demand increases | Evidence-based standard of care; 14 million procedures performed; measurable outcome improvements |
| Decision Making | Surgeon-directed with passive robotic assistance; no AI involvement; manual planning | 3D visualization enhances decision-making; pre-operative CT planning integrated | AI-powered real-time guidance; force feedback provides tactile information; autonomous task capability demonstrated |
| Misinformation | Overly optimistic predictions of robot replacement; public fear of autonomous surgery | Marketing claims sometimes outpaced evidence; costs underreported to patients | Hype around autonomous surgery persists despite expert caution; competitive claims require scrutiny |
| Service Delivery | Single procedures in single specialties; long operating times; experimental outcomes | Multi-specialty application; shorter recovery times; 15% of general surgery procedures by 2020 | 900,000 annual procedures in US; expanding into cardiac surgery; telesurgery across 286 km demonstrated |
| Accountability | Research ethics boards oversee experimental use; no regulatory framework specific to robotic surgery | FDA clearance process established; adverse event reporting systems created | AI liability questions emerge; data privacy concerns from cloud-connected systems; access equity debates intensify |
Real-World Examples
The Cleveland Clinic implemented a comprehensive robotic surgery program across multiple surgical specialties, deploying da Vinci Xi systems for urological, gynecological, and general surgical procedures. According to institutional data published through Intuitive Surgical's outcomes database, the program achieved a conversion rate to open surgery below 2 percent and demonstrated a 40 percent reduction in average hospital length of stay for robotic prostatectomy compared to open approaches. The measurable outcomes included reduced blood loss, fewer transfusions, and faster return to continence and potency for prostatectomy patients. Critics have noted that Cleveland Clinic's results reflect the performance of high-volume expert surgeons and may not be generalizable to community hospitals with lower surgical volumes and less experienced operators.
India's SS Innovations developed the SSI Mantra surgical robotic system as an indigenously manufactured alternative to imported platforms, performing the first robotic cardiac surgery in the Americas using its SSI Mantra 3 system at Interhospital in Ecuador in June 2025. The system has been installed in 80 hospitals across India and other countries, with the company aiming for FDA clearance in 2026. The key measurable outcome was demonstrating that a robotic surgical system could be manufactured outside the traditional Western supply chain at a fraction of the cost of da Vinci systems. The limitation is that SSI Mantra's published clinical evidence base remains far smaller than Intuitive Surgical's, and long-term comparative outcome data against established platforms is not yet available.
CMR Surgical's Versius system was adopted across 20 NHS hospitals in the United Kingdom, completing over 20,000 procedures by March 2024 and achieving regulatory approval in multiple countries including Australia, India, and several European and Latin American nations. The system's modular, compact design allowed installation in operating theaters that could not physically accommodate the larger da Vinci platform. The measurable outcome was demonstrating that competitive robotic systems could achieve clinical adoption at scale within a national healthcare system. The limitation is that Versius does not yet offer the same breadth of specialized instruments and established training infrastructure that the da Vinci ecosystem provides, creating a gap in capability for complex procedures.
Case Studies
Sutter Health and ROBODOC's Historic First
Sutter Medical Center in Sacramento faced the challenge of improving the precision of femoral cavity preparation during hip replacement surgery, where manual techniques produced inconsistent results that affected implant longevity. Dr. William Bargar and veterinarian Hap Paul developed ROBODOC through Integrated Surgical Systems with IBM, creating a system that could pre-plan operations using CT imaging and execute bone milling with robotic precision. On November 7, 1992, ROBODOC performed its first human hip replacement at Sutter General Hospital, successfully replacing the hip of a 64-year-old osteoarthritis patient in what Newsweek reported came off without a complication. The measurable impact included demonstrated proof that active robotic surgery on bone was safe and effective, spurring a worldwide trend toward robotic-assisted orthopedic procedures. ROBODOC gained acceptance in Europe with thousands of procedures performed, though it did not initially receive FDA marketing clearance in the United States due to concerns about complication rates relative to manual techniques.
Operation Lindbergh and Transatlantic Telesurgery
Surgeon Jacques Marescaux and his team confronted the question of whether surgical skill could be delivered across geographic distances through robotic telemanipulation, a capability that DARPA had envisioned for battlefield medicine. Using the ZEUS Robotic Surgical System and a dedicated fiber-optic connection between New York and Strasbourg, France, Marescaux performed a cholecystectomy on a patient more than 3,800 miles away in September 2001. The measurable impact was proving that transatlantic robotic telesurgery was technically feasible, with acceptable latency over a dedicated high-speed connection. The procedure received global media coverage and demonstrated the potential for expert surgical care to be delivered to patients regardless of their physical location. The limitation was that the dedicated network infrastructure required to achieve acceptable latency was prohibitively expensive and impractical for routine clinical use, and no regulatory framework existed for cross-border surgical practice.
Intuitive Surgical's Cardiac Surgery Expansion
Intuitive Surgical confronted the challenge of expanding its da Vinci platform beyond its established strongholds in urology, gynecology, and general surgery into the technically demanding field of cardiac surgery. The company received FDA clearance for nine new cardiac indications in 2025, including mitral and tricuspid valve repair, mitral valve replacement, and left atrial appendage closure, and began planning a limited U.S. rollout with specialized training programs for cardiac surgical teams in 2026. The measurable impact was demonstrating that robotic-assisted cardiac surgery could eliminate sternotomy entirely for certain valve procedures, dramatically reducing surgical trauma and recovery times. The da Vinci 5's force feedback, advanced imaging, and AI integration were positioned as critical enablers for cardiac applications where tissue sensitivity and anatomical complexity demand capabilities beyond what previous generations could provide. The criticism is that cardiac robotic surgery remains in its early adoption phase, and the long learning curve required for cardiac teams raises questions about whether complication rates during the ramp-up period will be acceptable to patients and hospital administrators.
Frequently Asked Questions About the First Robotic Surgery
The first robotic surgery was performed in 1985 at Memorial Medical Center in Long Beach, California. The PUMA 560 robotic arm, originally designed for industrial assembly, was used to perform a CT-guided stereotactic brain biopsy. The robot achieved sub-millimeter accuracy that eliminated the hand tremor errors that plagued neurosurgical needle placement at that time.
The first robot used in surgery was the PUMA 560, manufactured by Unimation for industrial applications and adapted for neurosurgical use. Its name stood for Programmable Universal Machine for Assembly, reflecting its factory-floor origins rather than any medical purpose. Researchers recognized its potential for eliminating unwanted motion during delicate procedures requiring extreme precision.
ROBODOC performed its first human surgery on November 7, 1992, at Sutter General Hospital in Sacramento, California. The patient was a 64-year-old man with osteoarthritis who received a robotic-assisted hip replacement. The surgery was developed by orthopedic surgeon Dr. William Bargar and veterinarian Hap Paul through Integrated Surgical Systems.
The FDA cleared the da Vinci Surgical System on July 11, 2000, for general laparoscopic surgical procedures. It was first cleared by the FDA in 1997 for assisting in surgery, and the 2000 approval expanded clearance to performing actual surgery. The system was developed by Intuitive Surgical and was the first robotic surgical system approved for multi-specialty use.
Over 14 million robotic-assisted procedures have been performed globally since the technology's inception. In the United States alone, nearly 900,000 robotic procedures are performed annually. The da Vinci system, installed in more than 7,500 hospitals across 69 countries, dominates the global robotic surgery landscape with a 70 to 80 percent market share.
Robotic surgery offers several documented advantages including reduced blood loss (up to 72 percent less in prostatectomy), lower surgical site infection rates (50 percent reduction in hysterectomy), shorter hospital stays (1.5 days less in colorectal surgery), faster patient recovery, and smaller incisions. The 3D visualization magnifies tissues up to 10 times, and instruments provide greater range of motion than the human wrist.
Da Vinci systems cost between $1.5 million and $2.5 million for initial purchase, with annual maintenance contracts of $80,000 to $170,000 and disposable instrument costs of $1,800 to $4,600 per procedure. Newer competitors like CMR Surgical's Versius offer systems at $1 to $1.5 million, and leasing models that represent about 40 percent of new placements reduce the upfront capital requirement.
The da Vinci 5 is the fifth generation of Intuitive Surgical's robotic platform, featuring over 150 design innovations and 10,000 times the computing power of its predecessor. Its most significant advancement is force feedback technology, allowing surgeons to feel tissue tension for the first time in the platform's history. Early data shows surgeons apply up to 43 percent less force on tissue with this feature.
Currently, surgical robots do not perform surgery independently. A human surgeon controls every movement from a console, and the robot translates those inputs into precise instrument actions. Researchers have demonstrated AI-enabled autonomous surgical tasks on animal tissue, but fully autonomous surgery on humans remains years away due to technical, ethical, and regulatory barriers.
Telesurgery involves a surgeon operating robotic instruments on a patient from a remote location. The first transatlantic telesurgery, Operation Lindbergh, was performed in 2001 between New York and Strasbourg using the ZEUS system. In January 2025, India's SSI Mantra performed telesurgeries over 286 kilometers with only 40-millisecond latency, demonstrating the technology's viability.
Urology and gynecology historically dominated robotic surgery, with prostatectomy and hysterectomy accounting for over 70 percent of procedures by 2010. General surgery has become the fastest-growing specialty for robotic adoption, and cardiac surgery is emerging as a new frontier with nine new FDA indications cleared for da Vinci in 2025.
Risks include the learning curve for surgeons (requiring 20 to 50 supervised cases for proficiency), potential for mechanical malfunction, and higher facility costs compared to laparoscopic surgery. The conversion rate from robotic to open surgery ranges from 0.8 to 5 percent. Some comparative studies show limited long-term outcome differences between robotic and well-performed laparoscopic surgery.
Robotic surgery progressed from a single brain biopsy in 1985 through urological (PROBOT, 1988), orthopedic (ROBODOC, 1992), and multi-specialty applications (da Vinci, 2000). Five generations of the da Vinci system added 3D visualization, dual consoles, overhead arms, single-port capability, and force feedback. AI integration and competitive systems from Medtronic, CMR, and others define the current landscape.
Market analysts project significant cost reductions as Intuitive Surgical's patents expire and new competitors enter the market. The global robotic surgery market is forecast to grow from $13.79 billion in 2025 to over $63 billion by 2035. Lower-cost systems from CMR Surgical, SSI Mantra, and others, combined with leasing and pay-per-use models, are expected to expand access to hospitals of all sizes and geographies.
AI currently enhances robotic surgery through real-time video analysis that identifies anatomical structures, predictive analytics for tissue characterization, and performance tracking for surgeon training. The da Vinci 5 leverages cloud connectivity for global data analysis and personalized coaching. Future applications include autonomous suturing, AI-guided surgical planning, and digital twin simulations of patient-specific procedures.
The answer depends on the specific procedure and surgeon experience. Robotic surgery offers advantages in visualization, instrument dexterity, and ergonomics for the surgeon, particularly in procedures requiring fine suturing or access to confined spaces. For simpler procedures like routine cholecystectomy, the benefits of robotic over laparoscopic approaches may be marginal, and the added cost may not be justified.