Introduction
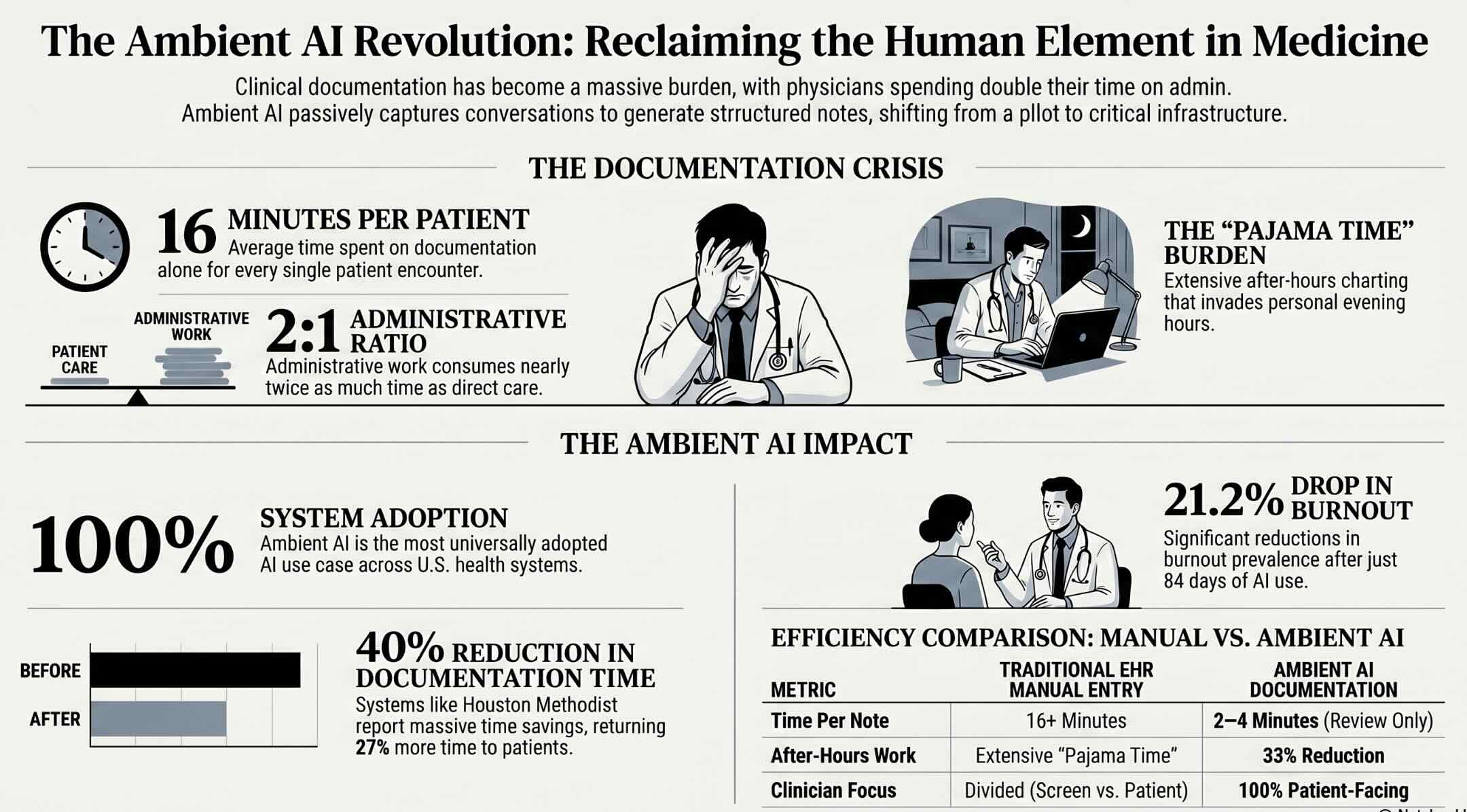
Clinical documentation consumes more physician time than any other single activity in modern healthcare, and artificial intelligence is now transforming this burden into an opportunity for better care, reduced burnout, and improved financial performance. Ambient AI documentation tools powered by generative AI have become the most universally adopted AI use case among healthcare systems, with 100 percent of health systems reporting some usage according to the American Medical Association’s latest data. Nearly two-thirds of U.S. hospitals using Epic electronic health records have adopted ambient AI tools, making AI-powered documentation the first clinical AI category to reach broad enterprise-scale deployment across the industry. A Mass General Brigham and UCSF multi-site study tracking ambient documentation across five U.S. hospitals for over two years found that clinicians using AI scribes in more than fifty percent of visits experienced the greatest reductions in documentation burden. AI in healthcare documentation has moved from pilot curiosity to operational infrastructure faster than any previous clinical technology, driven by the urgent need to return physician time from screens to patients. Houston Methodist reported that ambient AI reduced documentation time by forty percent, increased time spent with patients by twenty-seven percent, and cut after-hours charting by thirty-three percent across their deployment. This guide examines how AI documentation systems work, what measurable outcomes they deliver, and how healthcare organizations can deploy them responsibly across clinical settings.
Key Questions
What is AI healthcare documentation?
AI healthcare documentation uses ambient listening, natural language processing, and generative AI to automatically capture physician-patient conversations and generate structured clinical notes inside electronic health records without manual typing or dictation.
How does ambient AI documentation work?
Ambient AI passively listens to clinical encounters through microphones, transcribes the conversation in real time, extracts clinical details including diagnoses, medications, and plans, and generates a structured note for physician review and approval.
Does AI documentation reduce physician burnout?
Studies show AI documentation reduces burnout prevalence by up to 21.2 percent, cuts after-hours charting by 33 percent, saves clinicians 14 minutes per day on note writing, and increases documentation-related wellbeing by over 30 percent at major health systems.
Key Takeaways
- AI scribes generate draft clinical notes from natural conversation, but physician review, editing, and approval remain essential for accuracy, liability, and patient safety.
- Ambient AI documentation tools are the most adopted clinical AI use case, with 100 percent of health systems reporting some usage and nearly two-thirds of Epic hospitals deploying them.
- Physicians using AI documentation save up to 40 percent of documentation time, gain 27 percent more time with patients, and reduce after-hours charting by 33 percent.
- Mass General Brigham research shows 21.2 percent reduction in burnout prevalence after 84 days of ambient AI use, with Emory seeing 30.7 percent improvement in documentation-related wellbeing.
Table of contents
- Introduction
- Key Questions
- Key Takeaways
- What AI-Powered Healthcare Documentation Means?
- Why Documentation Has Become Healthcare’s Biggest Burden
- How Ambient AI Documentation Technology Works
- Measurable Outcomes from Major Health System Deployments
- Specialty-Specific Documentation Challenges and Solutions
- Clinical Documentation Integrity and Coding Accuracy
- Voice AI and Conversational Interfaces for Documentation
- Patient Consent, Privacy, and Data Protection
- Accuracy, Liability, and the Human Review Imperative
- AI Documentation for Nursing and Allied Health Professionals
- The EHR Integration Challenge
- Workforce Impact and Change Management
- The Future of AI-Powered Clinical Documentation
- Key Insights
- Real-World Examples
- Case Studies
- Frequently Asked Questions
What AI-Powered Healthcare Documentation Means?
AI-powered healthcare documentation refers to the application of ambient listening technology, natural language processing, speech recognition, and generative AI to automatically capture, transcribe, structure, and generate clinical notes from physician-patient encounters without requiring manual typing, dictation templates, or retrospective charting after visits. These systems passively listen to clinical conversations, extract relevant medical information including diagnoses, medications, procedures, allergies, and care plans, and produce structured documentation formatted to institutional standards within electronic health record systems. The technology transforms documentation from a manual task that competes with patient care into an automated process that happens naturally during the clinical encounter itself.
Why Documentation Has Become Healthcare’s Biggest Burden
Physicians entering medicine to care for patients instead spend the majority of their working hours interacting with screens, keyboards, and electronic health record systems rather than the people they trained to help. Research examining physician workflow found that documentation and administrative work consume nearly twice as much time as direct patient care, creating a structural imbalance that drives frustration and burnout. The average physician spends approximately sixteen minutes per patient encounter on documentation alone, with additional time required for after-hours charting that clinicians call “pajama time” because it invades personal evening hours. Electronic health records, while improving data access and coordination, dramatically increased the documentation burden by requiring structured data entry, click-through templates, and compliance documentation that paper records never demanded. The documentation crisis is not a technology problem that better typing skills can solve but a structural flaw where clinical workflows demand more writing than caring, making AI intervention a necessity rather than a convenience. Physician burnout has reached epidemic proportions, with documentation burden consistently cited as a primary contributing factor that drives clinicians to reduce hours, change specialties, or leave medicine entirely. Understanding how artificial intelligence works at a foundational level helps healthcare leaders evaluate which documentation AI tools use genuine intelligence versus those that simply rebrand conventional dictation software.
The financial consequences of documentation burden extend beyond clinician satisfaction into organizational revenue, quality measurement, and regulatory compliance that depend on accurate, complete clinical records. Incomplete or inaccurate documentation causes coding errors that lead to claim denials, undercoding that reduces reimbursement, and compliance violations that trigger audit penalties across healthcare organizations. Quality reporting programs require specific documentation elements that busy clinicians frequently omit, resulting in lower quality scores and reduced payment under value-based care contracts. Referring physicians, care coordinators, and patients all depend on documentation quality for care continuity, yet the time pressure on documentation compromises the very records these stakeholders rely upon for clinical decision-making. Exploring the broader impact of AI on the healthcare sector reveals how documentation improvement connects to clinical quality, financial performance, and patient safety outcomes. The scale of the problem, affecting every physician in every specialty at every institution, makes documentation automation one of healthcare’s most impactful AI applications.
How Ambient AI Documentation Technology Works
The documentation burden creates the demand, and ambient AI technology provides the solution through a pipeline that converts natural clinical conversation into structured medical records automatically. The system begins when a physician activates the ambient listener, typically through a smartphone app, tablet, or workstation microphone positioned to capture the encounter between clinician and patient. Advanced speech recognition models transcribe the conversation in real time, distinguishing between physician and patient voices, handling medical terminology, accents, and conversational interruptions with increasing accuracy. Natural language processing engines analyze the transcript to extract clinical entities including symptoms, diagnoses, medications, dosages, procedures, allergies, and care plan elements from conversational language. The core innovation of ambient AI documentation is that it works within the natural flow of clinical care rather than requiring clinicians to change how they practice, speak, or interact with patients. Generative AI models then compose a structured clinical note organized according to institutional documentation standards, formatting extracted information into appropriate sections like history of present illness, assessment, and plan. Understanding what NLP is and how it processes language helps clinicians appreciate the linguistic AI powering the systems that convert their conversations into medical records.
The generated note appears in the electronic health record for physician review, editing, and approval before becoming part of the permanent medical record and triggering downstream processes. Physicians review AI-generated drafts for accuracy, adding clinical reasoning, correcting misinterpretations, and ensuring the note reflects their professional judgment about the encounter. Integration with electronic health record systems varies by vendor, with some ambient tools operating as standalone applications while others embed directly within Epic, Cerner, or other EHR platforms natively. Speaker diarization technology identifies who said what during multi-party encounters, distinguishing physician statements from patient statements and from family members or interpreters present during the visit. The system learns institutional preferences including note format, section organization, abbreviation conventions, and documentation style through configuration and ongoing usage feedback. These technical capabilities combine to produce a documentation workflow where the physician focuses entirely on the patient while the AI handles the recording, structuring, and formatting that previously consumed hours of clinical time.
Measurable Outcomes from Major Health System Deployments
Technology capabilities translate into outcomes, and the evidence from major health system deployments demonstrates measurable improvements in time savings, burnout reduction, and clinical workflow efficiency. Houston Methodist deployed ambient AI across ambulatory, emergency, and inpatient settings, reporting a forty percent reduction in documentation time, a twenty-seven percent increase in patient-facing time, and a thirty-three percent cut in after-hours charting work. Emory Healthcare saw a 30.7 percent increase in documentation-related wellbeing prevalence among clinicians using ambient documentation technology, documented in a study published in JAMA in 2025. Mass General Brigham observed a 21.2 percent reduction in burnout prevalence after eighty-four days of ambient AI utilization, with the greatest benefits among clinicians who used the technology in the majority of their encounters. The evidence from multi-site deployments confirms that ambient AI documentation delivers clinically significant reductions in burnout and meaningful time savings that compound across thousands of daily encounters. Cleveland Clinic found that AI Scribe from Ambience decreased the average time clinicians spent writing and reviewing notes by fourteen minutes per day across participating physicians. Intermountain Health saw a twenty-seven percent reduction in time spent on notes per appointment when using Dragon Copilot for clinicians who used the solution across ten or more encounters.
Cooper University Healthcare implemented Dragon Copilot and found the solution saved clinicians 4.15 minutes in documentation time per patient, accumulating to approximately one hour or more saved daily per physician across clinical sessions. Mercy Health experienced significant improvements in bedside time for nurses after implementing ambient documentation, demonstrating that AI documentation benefits extend beyond physician workflows into nursing practice. The Doximity 2026 State of AI in Medicine Report found that twenty-nine percent of physicians use voice-based documentation tools including ambient listening and AI scribes, up from twenty percent the previous year. Among physicians who adopt AI documentation, sixty-nine percent report using it daily, with thirty-six percent using it multiple times per day, indicating strong satisfaction that drives habitual adoption. Exploring how automation impacts healthcare operations provides broader context for how documentation AI fits within the wider transformation of clinical and administrative workflows. These measurable outcomes from dozens of major health systems provide the evidence base that justifies enterprise-wide deployment rather than continued pilot-scale experimentation.
Ambient AI ROI Calculator
The Role of AI in Healthcare Documentation
Estimate how ambient AI documentation could reduce charting burden and recover clinician capacity.
Estimated annual impact
AI documentation opportunity
Specialty-Specific Documentation Challenges and Solutions
Enterprise-wide deployment reveals that documentation needs vary dramatically across medical specialties, requiring AI systems that adapt to different clinical workflows, terminology, and note structures. Primary care encounters involve broad differential diagnoses, medication reconciliation across multiple conditions, preventive care documentation, and care coordination notes that require comprehensive but concise documentation covering diverse topics. Surgical specialties demand precise procedural documentation including operative notes that describe technical details, anatomical findings, and complications with exacting specificity. Mental health documentation presents unique challenges because therapeutic conversations contain sensitive content, subjective assessments, and relationship dynamics that require careful handling by AI systems. Effective ambient AI documentation must adapt to the fundamentally different documentation patterns across specialties rather than applying a one-size-fits-all approach that works well for primary care but fails in surgical, emergency, or psychiatric contexts. Emergency medicine requires rapid documentation across high-acuity, time-pressured encounters where multiple patients are managed simultaneously and clinical situations change rapidly. Understanding how deep learning powers healthcare AI helps clinicians grasp why modern AI documentation systems can adapt to specialty-specific language patterns that earlier rule-based systems could not handle.
Radiology generates documentation from image interpretation rather than patient conversation, requiring AI systems that assist with structured reporting from imaging findings rather than ambient conversation capture. Pathology documentation involves microscopic findings, specimen descriptions, and diagnostic classifications that follow highly standardized formats with specific terminology requirements. Pediatric encounters include documentation of developmental milestones, growth parameters, parental concerns, and vaccine histories alongside standard clinical notes, adding complexity that adult-focused AI models may miss. Cardiology documentation demands precise recording of vital signs, waveform interpretations, hemodynamic data, and procedure-specific details that combine narrative description with quantitative measurements. These specialty variations mean that ambient AI platforms must either offer specialty-specific models or maintain sufficient flexibility to adapt their output formats, vocabulary, and documentation patterns to each clinical context.
Clinical Documentation Integrity and Coding Accuracy
Specialty documentation connects directly to financial performance, where AI improves not just the speed of documentation but the accuracy and completeness that determine coding quality and reimbursement levels. Clinical documentation integrity programs use AI to review physician notes in real time, identifying opportunities to improve specificity, capture severity indicators, and document conditions that affect coding accuracy. Natural language processing analyzes free-text clinical narratives and suggests more specific diagnostic terminology, ensuring that documentation supports the highest appropriate code rather than defaulting to less specific alternatives. AI coding assistance bridges the gap between clinical language physicians use naturally and the coding language that billing systems require, reducing the manual translation work that dedicated coding professionals perform. AI-powered clinical documentation integrity programs simultaneously improve care quality through more precise documentation and financial performance through more accurate coding, aligning clinical and business objectives rather than forcing tradeoffs. Computer-assisted coding systems translate physician documentation into appropriate medical codes by understanding clinical context, terminology variations, and specialty-specific documentation patterns automatically. Exploring how RPA helps healthcare operations demonstrates how documentation AI integrates with broader revenue cycle automation to deliver end-to-end financial process improvement.
Query generation systems identify documentation gaps that could affect coding accuracy and generate physician queries requesting specific clarification before records are finalized and coded. Severity of illness and risk of mortality indicators depend on documentation specificity, meaning that AI improvements in clinical documentation directly affect the case mix index that determines hospital reimbursement rates. Compliance monitoring uses AI to review documentation patterns against audit benchmarks, identifying potential overcoding or undercoding trends that could trigger regulatory scrutiny or represent revenue leakage. Quality measure abstraction automates the extraction of clinical quality indicators from documentation, reducing the manual chart review burden that quality departments face during regulatory reporting periods. Understanding how AI transforms healthcare business processes reveals the revenue cycle connections that make documentation accuracy a financial priority alongside a clinical one. The financial impact of improved documentation accuracy is substantial because coding specificity improvements of even a few percentage points across thousands of encounters translate into millions of dollars in additional appropriate reimbursement.
Voice AI and Conversational Interfaces for Documentation
Coding accuracy builds on the voice technology foundation, where conversational AI interfaces expand documentation capabilities beyond ambient listening into interactive clinical assistants that respond to physician commands. Voice-commanded documentation allows physicians to dictate notes, navigate electronic health records, place orders, and access clinical information through natural speech rather than keyboard and mouse interaction with computer systems. Conversational AI assistants answer clinical questions, retrieve patient history, summarize prior encounters, and provide decision support through spoken dialogue that integrates with documentation workflows seamlessly. Multilingual voice AI enables documentation in multiple languages, supporting physicians who practice in diverse communities and patients who communicate in languages other than English during clinical encounters. Voice AI transforms the electronic health record from a barrier between physician and patient into a responsive assistant that operates through natural speech, preserving the clinical relationship while handling documentation simultaneously. Virtual nursing assistants use voice AI to document patient assessments, vital signs, medication administration, and care activities through conversational interfaces that reduce the screen-based documentation burden affecting nursing workflows. Examining how voice AI transforms contact center operations reveals the same conversational technologies adapted for clinical documentation contexts.
Speech-to-text accuracy for medical terminology has improved dramatically with domain-specific language models trained on millions of clinical encounters across dozens of specialties and hundreds of medical conditions. Noise cancellation and environmental filtering enable voice AI to operate accurately in clinical settings including busy emergency departments, shared workspaces, and operating rooms where background noise challenges consumer-grade speech recognition. Wake word detection and privacy controls ensure that voice AI captures only authorized clinical conversations, preventing accidental recording of non-clinical discussions and maintaining appropriate boundaries around surveillance concerns. Voice biometric authentication verifies physician identity through speech patterns, adding a security layer that ensures documentation is attributed to the correct provider without requiring separate login procedures. These voice capabilities represent the natural evolution of documentation AI from passive ambient listening toward active clinical assistance that supports physicians throughout their entire workflow.
Patient Consent, Privacy, and Data Protection
Voice technology captures sensitive clinical conversations, making patient consent and data protection essential governance requirements that healthcare organizations must address before deploying ambient documentation AI. Patient notification and consent processes vary by jurisdiction and institution, with some requiring explicit opt-in consent before recording conversations while others provide opt-out notification with assumed consent. HIPAA requirements govern how recorded conversations, transcripts, and AI-generated notes are stored, accessed, transmitted, and retained as protected health information within covered entity systems. Data residency requirements may restrict where clinical conversation data is processed and stored, affecting which cloud-based AI platforms healthcare organizations can use for ambient documentation. Patient trust in healthcare depends on the assurance that clinical conversations remain confidential, making transparent consent processes and robust data protection essential prerequisites for AI documentation adoption rather than afterthoughts. De-identification protocols remove patient-identifying information from conversation data used for AI model improvement, ensuring that training processes do not expose individual health information beyond the clinical encounter that generated it. Understanding AI data privacy and security challenges provides broader context for the privacy frameworks essential when AI systems process some of the most sensitive personal information that exists.
Third-party vendor risk assessments evaluate how ambient AI providers handle, store, and process clinical conversation data, examining business associate agreements, security certifications, and breach notification capabilities. Audit trail requirements ensure that AI-generated documentation maintains records of who approved, edited, or modified notes, preserving the accountability chain that medical record integrity requires. Data retention policies must balance the value of conversation recordings for quality improvement and dispute resolution against the privacy risks of maintaining extended recordings of intimate clinical discussions. International data transfer considerations affect healthcare organizations using cloud-based AI platforms that may process clinical data across jurisdictions with varying privacy protection standards. Building responsible AI governance frameworks provides structured approaches for healthcare organizations establishing the privacy policies that ambient AI documentation deployment requires. These privacy protections are not barriers to innovation but necessary foundations that sustain the patient trust upon which effective healthcare delivery depends.
Accuracy, Liability, and the Human Review Imperative
Privacy governance connects to clinical accountability, where the accuracy of AI-generated documentation and the liability for errors create legal and professional obligations that shape deployment practices. AI-generated clinical notes contain errors that physicians must identify and correct during review, including misattributed statements, incorrect medical terminology, hallucinated clinical details, and missed information from conversations. The rate of clinically significant errors in AI-generated documentation varies by specialty, encounter complexity, and AI platform, requiring ongoing quality monitoring that many organizations have not yet formalized. Medical malpractice liability for documentation errors in AI-generated notes remains with the signing physician, meaning that cursory review of AI drafts creates legal risk that adequate review processes must mitigate. The physician's signature on an AI-generated note carries the same legal and professional weight as a manually written note, making thorough review not optional but a non-negotiable professional obligation. Note bloat, where AI-generated documentation includes unnecessary detail, repetitive content, or template language that obscures clinically important information, represents a quality concern distinct from factual accuracy. Exploring which careers AI cannot easily replace reinforces why physician judgment in reviewing AI-generated documentation remains irreplaceable despite the technology's impressive capabilities.
Standardized review workflows train physicians to efficiently verify AI-generated notes, focusing attention on high-risk sections like medication lists, allergies, assessment, and plan where errors carry the greatest clinical consequences. Quality assurance programs compare AI-generated notes against physician-edited final versions, identifying systematic error patterns that inform model improvements and targeted reviewer training. Institutional policies defining acceptable AI documentation use, review responsibilities, and correction procedures protect both patients and physicians by establishing clear expectations and accountability frameworks. The tension between time savings and thorough review requires organizations to find the balance where AI documentation reduces overall burden without creating new risks from inadequate verification. Malpractice insurers are developing guidance on AI documentation liability, though the legal landscape remains evolving as courts address cases involving AI-assisted clinical records for the first time. Organizations that establish robust review protocols, quality monitoring, and clear liability frameworks position themselves to capture AI documentation benefits while managing the risks that hasty adoption without governance creates.
AI Documentation for Nursing and Allied Health Professionals
Physician-focused discussion overlooks nursing and allied health professionals, who face documentation burdens equally severe and stand to benefit substantially from AI tools tailored to their specific workflow requirements. Nurses spend approximately twenty-five percent of their shift time on documentation, recording assessments, vital signs, medication administration, care activities, and patient education across multiple patients simultaneously. Ambient AI for nursing captures bedside assessments, handoff communications, and patient interactions, generating documentation that nurses currently enter manually into electronic health records between patient care activities. Mercy Health reported significant improvements in bedside time after implementing ambient documentation for nurses, demonstrating that AI documentation benefits extend beyond physician workflows into nursing practice meaningfully. Nursing documentation AI addresses the paradox where the professionals closest to patients spend the most time documenting care rather than delivering it, directly affecting both nurse satisfaction and patient safety outcomes. Physical therapy, occupational therapy, and speech therapy documentation involves detailed functional assessments, treatment descriptions, and progress measurements that consume significant time these professionals could redirect toward patient treatment. Understanding how AI enhances predictive analytics reveals the same pattern recognition capabilities that enable nursing AI to identify documentation patterns and automate routine recording tasks.
Home health documentation requires clinicians to record detailed assessments, care plans, and visit notes in settings without the technology infrastructure available in hospital environments. Behavioral health documentation involves sensitive therapeutic observations, safety assessments, and treatment planning that require AI systems designed with appropriate privacy safeguards and clinical judgment boundaries. Pharmacy documentation for medication reconciliation, clinical interventions, and patient counseling generates records that AI can assist with by extracting relevant information from patient interactions. Social work documentation records psychosocial assessments, resource referrals, and care coordination activities that AI can streamline while preserving the nuanced professional observations these records require. These allied health applications represent substantial untapped potential because most ambient AI development has focused on physician encounters, leaving nursing and therapy documentation largely unaddressed by current commercially available solutions.
The EHR Integration Challenge
Allied health deployment depends on EHR integration, which represents both the critical enabler and the most significant technical barrier to enterprise-scale ambient AI documentation deployment. Ambient AI documentation must integrate seamlessly with electronic health record systems to deliver notes directly into patient charts without requiring manual copy-paste workflows that negate time savings. Epic's broad availability of ambient AI functionality to its client hospitals has accelerated adoption, with nearly two-thirds of Epic hospitals implementing ambient documentation through the platform's native integration. Cerner, Oracle Health, MEDITECH, and other EHR vendors offer varying levels of ambient AI integration, with some requiring third-party middleware that adds complexity and potential failure points to documentation workflows. The hospital that achieves seamless AI-to-EHR integration gains compounding returns because every clinical encounter generates documentation that flows directly into the coding, billing, quality, and analytics systems that depend on structured clinical data. API-based integrations connect ambient AI platforms to EHR systems through standardized interfaces, though performance depends on the maturity and completeness of each EHR vendor's API ecosystem. Exploring how big data serves the healthcare sector reveals the data infrastructure requirements that AI documentation systems depend upon for effective integration and analytics.
Template mapping ensures that AI-generated notes populate the correct fields, sections, and data elements within EHR documentation templates specific to each specialty and encounter type. Discrete data extraction converts narrative clinical text into structured data elements including problem lists, medication lists, and order entries that EHR systems use for clinical decision support and analytics. Interoperability standards through FHIR and HL7 facilitate data exchange between ambient AI platforms and EHR systems, though implementation maturity varies significantly across vendors and health systems. Single sign-on integration ensures that physicians access ambient AI tools through their existing EHR authentication, preventing additional login steps that create friction and reduce adoption rates. These integration challenges are solvable but require dedicated technical resources, vendor collaboration, and organizational commitment that distinguish successful deployments from pilot projects that stall at the integration phase.
Workforce Impact and Change Management
Integration success depends on workforce readiness, where change management determines whether AI documentation tools are embraced as productivity enhancers or resisted as threatening disruptions to established clinical workflows. Medical scribes who currently document physician encounters face role evolution as AI ambient technology replaces the transcription function that defines their position in clinical workflows. Rather than elimination, scribe roles may evolve toward quality review, AI output verification, patient engagement support, and clinical coordination functions that leverage their healthcare knowledge. Physician adoption rates correlate with perceived ease of use, time savings, and note quality, meaning that tools producing inferior output or requiring excessive review fail regardless of institutional mandate or executive enthusiasm. Successful AI documentation deployment requires treating the technology as a workflow transformation rather than a software installation, investing in training, feedback loops, and cultural adaptation alongside technical implementation. Medical education must prepare future physicians to work with AI documentation tools, teaching critical review skills, understanding of AI limitations, and appropriate reliance that current curricula largely ignore. Understanding AI and the future of work helps healthcare leaders contextualize documentation AI within the broader workforce transformation affecting every clinical and administrative role.
Champions and early adopters within clinical departments accelerate organizational adoption by demonstrating benefits, sharing workflows, and providing peer support that institutional training programs alone cannot replicate. Physician feedback mechanisms that route suggestions, error reports, and workflow concerns to AI vendors and institutional leaders create continuous improvement cycles that sustain adoption beyond initial enthusiasm. Governance committees including clinicians, informaticists, compliance officers, and patient representatives ensure that deployment decisions balance efficiency with quality, privacy, and equity considerations. Metric-based evaluation tracking time savings, note quality, physician satisfaction, patient experience, and financial impact provides the evidence needed to justify continued investment and identify areas requiring improvement. These change management practices distinguish organizations that successfully scale AI documentation from those that experience pilot fatigue and abandoned implementations after initial deployment.
The Future of AI-Powered Clinical Documentation
Change management prepares organizations for a future where AI documentation capabilities expand dramatically beyond current ambient listening into comprehensive clinical intelligence systems. Agentic AI documentation systems will not merely record encounters but proactively surface relevant patient history, suggest clinical actions, pre-populate orders, and coordinate follow-up care based on conversation content automatically. Multimodal documentation will integrate conversation capture with medical imaging, vital sign streams, wearable device data, and laboratory results into unified clinical records that synthesize multiple data sources. Real-time clinical decision support embedded within documentation workflows will alert physicians to drug interactions, guideline deviations, and diagnostic considerations during the encounter rather than after documentation is complete. The future of clinical documentation is not faster note-writing but intelligent clinical partnership where AI systems contribute to clinical reasoning alongside recording what occurred during each patient encounter. Predictive documentation will anticipate charting requirements based on scheduled patients, presenting pre-populated sections that physicians confirm or modify rather than creating from scratch for every encounter. Examining what generative AI means for healthcare reveals the foundational technology powering the next generation of documentation systems that will evolve from scribes to clinical partners.
Patient-generated documentation through AI-powered portals will enable patients to contribute symptom histories, medication updates, and concern descriptions that pre-populate encounter documentation before the visit begins. Cross-encounter synthesis will use AI to generate longitudinal patient summaries that track disease progression, treatment responses, and care milestones across multiple visits and providers automatically. Quality measurement will become continuous rather than retrospective as AI extracts performance indicators from documentation in real time, enabling immediate feedback on care quality and documentation completeness. Interoperability advances will enable AI documentation systems to incorporate information from external providers, pharmacies, laboratories, and health information exchanges into encounter records seamlessly. The convergence of ambient documentation, clinical decision support, and predictive analytics will transform the clinical note from a retrospective record into a forward-looking clinical tool that actively improves patient care.
Key Insights
- Cooper University Healthcare found Dragon Copilot saved 4.15 minutes per patient, accumulating to one hour or more saved daily per physician.
- Ambient AI documentation tools are the most universally adopted clinical AI, with 100 percent of health systems reporting some usage according to the American Medical Association.
- Nearly two-thirds of U.S. hospitals using Epic have adopted ambient AI documentation tools, with adoption associated with workload, financial performance, and hospital size.
- Houston Methodist reported ambient AI reduced documentation time by 40 percent, increased patient-facing time by 27 percent, and cut after-hours charting by 33 percent.
- Emory Healthcare saw a 30.7 percent increase in documentation-related wellbeing associated with ambient documentation use, per a JAMA-published study.
- Mass General Brigham observed a 21.2 percent reduction in burnout prevalence after 84 days of ambient AI utilization across their health system.
- Cleveland Clinic found that AI Scribe decreased average note-writing time by 14 minutes per day for participating physicians.
- The Doximity 2026 report found 29 percent of physicians use voice-based documentation tools, with 69 percent of adopters using them daily.
| Dimension | Manual Documentation | Traditional Dictation | Template-Based EHR | Ambient AI Documentation |
|---|---|---|---|---|
| Time Per Note | 16+ minutes manual typing | 8–12 minutes dictation plus editing | 10–15 minutes clicking through templates | 2–4 minutes physician review of AI draft |
| After-Hours Work | Extensive "pajama time" charting | Moderate dictation backlogs | Moderate template completion | 33% reduction in after-hours documentation |
| Patient Interaction | Physician divided between screen and patient | Physician dictates after encounter | Physician clicks during or after encounter | Physician focuses entirely on patient |
| Note Quality | Variable, dependent on physician effort | Transcription errors and formatting issues | Standardized but often copy-forward bloat | Structured, encounter-specific, reviewable |
| Burnout Impact | Major contributor to physician burnout | Modest reduction in typing burden | Template fatigue and click fatigue | 21–31% documented burnout and wellbeing improvements |
| Coding Accuracy | Variable, relies on physician coding awareness | Dependent on transcription accuracy | Template prompts improve specificity | AI suggests coding-relevant documentation elements |
| Scalability | Scales only with physician time | Requires transcription infrastructure | Limited by template design resources | Scales across specialties with model adaptation |
| Current Adoption | Declining as EHRs replace paper | Declining, replaced by AI voice tools | Universal through EHR platforms | 100% of health systems, 65% of Epic hospitals |
Real-World Examples
Houston Methodist Ambient AI System-Wide Deployment
Houston Methodist rolled out ambient AI documentation across ambulatory, emergency, and inpatient settings, becoming one of the first major health systems to deploy the technology across its entire clinical operation rather than limiting it to pilot departments. The system reduced documentation time by forty percent, increased time physicians spent with patients by twenty-seven percent, and cut after-hours charting work by thirty-three percent across deployed settings. Clinicians were able to close encounters faster and see more patients per day, generating measurable improvements in both provider experience and operational throughput across the health system. The deployment demonstrated that ambient AI scales effectively across different clinical environments, from outpatient clinics to emergency departments, when supported by adequate integration and training infrastructure. Limitations included the need for ongoing model tuning across different specialties and the challenge of maintaining consistent review quality as physicians became more comfortable and potentially less vigilant with AI-generated drafts. Houston Methodist's deployment is documented through ScienceSoft's healthcare AI trend analysis.
Mass General Brigham Multi-Site Burnout Study
Mass General Brigham and UCSF conducted the largest multi-site study of ambient AI documentation's impact on clinician workflows, tracking usage across five U.S. hospitals for more than two years with rigorous measurement methodology. The study found that clinicians who used ambient documentation in more than fifty percent of patient visits experienced the greatest reductions in documentation burden, establishing a dose-response relationship between usage frequency and benefit magnitude. Mass General Brigham observed a 21.2 percent reduction in burnout prevalence after eighty-four days of ambient AI utilization, providing the most rigorous evidence to date that AI documentation produces clinically meaningful wellbeing improvements. The research design provided stronger evidence than single-site studies by controlling for institutional variation, specialty differences, and individual physician factors that could confound burnout measurements. Limitations included the challenge of isolating ambient AI's specific contribution to burnout reduction from other concurrent wellness interventions and the relatively short follow-up period for assessing sustained impact. The study findings are published through EurekAlert/Mass General Brigham research communications.
Emory Healthcare JAMA-Published Wellbeing Improvement
Emory Healthcare deployed ambient documentation technology and conducted a rigorous study published in JAMA in 2025 measuring the association between ambient AI use and physician documentation-related wellbeing across participating clinicians. The study found a 30.7 percent increase in documentation-related wellbeing prevalence associated with ambient documentation technology use, representing one of the largest documented wellbeing improvements from any single clinical technology intervention. The JAMA publication provided peer-reviewed validation that ambient AI produces measurable, statistically significant improvements in physician experience metrics that the healthcare industry uses to track workforce sustainability. The Emory deployment demonstrated that wellbeing improvements extend across multiple specialties when ambient AI is deployed with adequate training, integration, and institutional support for adoption. Limitations included the observational study design, which establishes association rather than definitive causation, and the potential for selection bias if physicians most receptive to technology adopted ambient AI earlier. The study is documented through the AHA Center for Health Innovation.
Case Studies
Cleveland Clinic's AI Scribe Implementation
Cleveland Clinic faced the challenge of documentation burden consuming excessive physician time across its sprawling multi-hospital system, contributing to burnout and reducing the time clinicians could devote to direct patient care and complex clinical decision-making. Physicians reported that EHR documentation demands had steadily increased over the prior decade, with each regulatory requirement, quality metric, and billing specification adding documentation tasks without removing existing ones. Cleveland Clinic implemented AI Scribe from Ambience Healthcare, deploying ambient AI documentation across clinical departments to automatically generate draft notes from physician-patient conversations during encounters. The system captured clinical conversations, extracted relevant medical information, and produced structured notes formatted to Cleveland Clinic's institutional standards within the Epic EHR for physician review and finalization. The measurable impact included a decrease of fourteen minutes per day in the average time clinicians spent writing and reviewing notes in the EHR system, accumulating to significant time savings across the physician workforce. The limitation was that documentation time reduction varied across specialties, with procedure-heavy and complex multi-problem encounters showing less time savings than straightforward primary care visits where AI performed most effectively. Quality monitoring revealed that AI-generated notes occasionally included unnecessary detail or missed nuanced clinical reasoning that physicians needed to add manually during review, requiring ongoing feedback to improve model performance. Cleveland Clinic's deployment is documented through the AHA ambient AI scribe report.
Cooper University Healthcare Documentation Transformation
Cooper University Healthcare in Camden, New Jersey, identified clinician burnout as an organizational priority after survey data revealed documentation burden as the primary driver of physician dissatisfaction and turnover risk across the health system. The challenge was compounded by the competitive physician recruitment market in the greater Philadelphia region, where documentation-intensive practices risked losing talent to competitors offering better clinical workflows and work-life balance. Cooper implemented Dragon Copilot from Nuance, deploying ambient AI documentation across clinical departments with dedicated training, integration support, and quality monitoring from project launch through system-wide adoption. The system generated draft clinical notes from physician-patient conversations, with physicians reviewing and approving notes before they became part of the permanent medical record within the institutional EHR system. Measurable outcomes included 4.15 minutes saved per patient encounter in documentation time, accumulating to approximately one hour or more saved daily per physician, with associated improvements in clinician satisfaction scores. The limitation was that implementation required significant IT and change management resources, and some physicians with well-established dictation workflows resisted transitioning to ambient AI despite measured time savings for adopters. Concerns about AI note accuracy required establishing quality review protocols that added a new governance layer to clinical documentation processes that did not exist under previous manual documentation approaches. Cooper's implementation is documented through AHA health innovation reporting.
Ambient AI Adoption Equity Across U.S. Hospitals
Researchers studying ambient AI adoption patterns across U.S. hospitals identified that deployment was not distributed equally, with adoption concentrated among larger, metropolitan, nonprofit hospitals with stronger financial performance, raising equity concerns. Smaller, rural, publicly funded hospitals with tighter operating margins and higher staffing-adjusted workloads were less likely to have adopted ambient AI despite potentially benefiting most from documentation time savings. The study, published in the American Journal of Managed Care in 2026, used Epic Showroom data linked to American Hospital Association survey characteristics to analyze adoption determinants across a national sample of hospitals. Findings revealed that adoption was significantly associated with hospital size, metropolitan location, nonprofit ownership, operating margin strength, and geographic region, with lower adoption in the Midwest compared to the South. The research provided the first large-scale evidence that ambient AI documentation tools risk widening operational disparities between well-resourced and under-resourced hospitals if adoption barriers are not actively addressed. The limitation was that the cross-sectional design captured a single point in time during rapid adoption growth, meaning that current patterns may not reflect future steady-state adoption as costs decrease and evidence accumulates. Policy implications included the potential need for subsidized access programs, shared service models, or vendor pricing adjustments that enable smaller and rural hospitals to adopt ambient AI without the financial resources that early adopters leveraged. The research is published in the American Journal of Managed Care.
Frequently Asked Questions
AI-powered healthcare documentation uses ambient listening technology and generative AI to automatically capture physician-patient conversations and produce structured clinical notes within electronic health records. The system transcribes conversations, extracts clinical details including diagnoses, medications, and plans, and generates notes formatted to institutional standards for physician review. This eliminates manual typing and after-hours charting that contribute significantly to physician burnout.
Ambient AI activates through a microphone during clinical encounters, transcribes the conversation using medical speech recognition, and applies natural language processing to extract clinical entities from conversational speech. Generative AI then composes a structured clinical note organized according to specialty-specific documentation standards and delivers it to the EHR for physician review. The physician reviews, edits, and approves the note before it becomes part of the permanent medical record.
Multiple large-scale studies demonstrate measurable burnout reduction, including Mass General Brigham's 21.2 percent reduction in burnout prevalence after 84 days of use and Emory Healthcare's 30.7 percent increase in documentation-related wellbeing. Houston Methodist reported 33 percent reduction in after-hours charting and 27 percent more time with patients. These peer-reviewed findings from major health systems provide strong evidence that AI documentation produces clinically significant wellbeing improvements.
Cleveland Clinic found AI Scribe saved fourteen minutes per day in note-writing time, while Cooper University Healthcare measured 4.15 minutes saved per patient encounter, accumulating to one hour or more daily. Houston Methodist reported forty percent overall reduction in documentation time across ambulatory, emergency, and inpatient settings. Time savings vary by specialty, encounter complexity, and individual physician documentation habits.
AI-generated notes contain errors that physicians must identify during review, including misattributed statements, incorrect terminology, hallucinated details, and missed information from conversations. Accuracy varies by specialty, encounter complexity, and AI platform, with primary care encounters generally producing higher-quality drafts than complex multi-problem visits. Physician review and approval before note finalization remain essential for clinical accuracy and legal protection.
The signing physician bears malpractice liability for AI-generated documentation, meaning thorough review is a professional obligation rather than an optional convenience. Institutional policies must define acceptable AI documentation use, review responsibilities, and correction procedures to protect both patients and physicians. The legal landscape continues evolving as courts address cases involving AI-assisted clinical records.
Nearly two-thirds of U.S. hospitals using Epic electronic health records have adopted ambient AI documentation tools, and 100 percent of health systems report some usage of ambient documentation. Twenty-nine percent of physicians use voice-based documentation tools including ambient listening, with 69 percent of adopters using them daily. Adoption is growing rapidly across all specialties and practice settings.
AI documentation systems capture sensitive clinical conversations, requiring patient consent processes, HIPAA compliance, secure data storage, and clear policies about recording, retention, and use of conversation data. De-identification protocols protect patient information used for model improvement, and audit trails maintain accountability for who accessed, approved, or modified documentation. Privacy governance is a prerequisite for deployment rather than an afterthought.
AI documentation effectiveness varies across specialties, with primary care and general medicine encounters producing the highest-quality drafts and complex procedural or psychiatric encounters presenting greater challenges. Specialty-specific model training improves output quality, and platforms increasingly offer configurations tailored to surgical, emergency, behavioral health, and pediatric documentation requirements. Most vendors are actively expanding specialty coverage as the technology matures.
AI documentation improves coding accuracy by suggesting specific diagnostic terminology, capturing severity indicators, and ensuring documentation supports the highest appropriate code for each encounter. Clinical documentation integrity programs using AI review notes in real time, identifying coding-relevant documentation opportunities that physicians might otherwise miss. Improved documentation specificity directly increases appropriate reimbursement and reduces claim denial rates.
AI is transforming the medical scribe role rather than eliminating it entirely, shifting responsibilities from real-time transcription toward quality review, AI output verification, patient engagement, and clinical coordination. Organizations transitioning from human scribes to AI documentation often retain scribes in evolved roles that leverage their healthcare knowledge for higher-value functions. The transition timeline and scope depend on AI documentation quality, institutional preferences, and the specific value scribes provide beyond transcription.
Epic leads ambient AI integration with nearly two-thirds of its hospital clients deploying the technology natively within the platform. Oracle Health, MEDITECH, and other vendors offer varying levels of integration through native capabilities or third-party partnerships. FHIR-based APIs enable ambient AI platforms to connect with most modern EHR systems, though integration depth and performance vary significantly across vendors.
Implementation costs vary significantly based on vendor platform, deployment scale, EHR integration complexity, and organizational change management investment required for successful adoption. Cloud-based ambient AI services typically charge per-provider monthly subscription fees that scale with the number of clinicians using the system. ROI calculations must include time savings, reduced after-hours costs, improved coding accuracy, burnout reduction, and retention benefits alongside direct technology costs.
Research shows ambient AI adoption is concentrated among larger, metropolitan, nonprofit hospitals with stronger financial performance, raising concerns about widening operational disparities for smaller and rural institutions. Cost barriers, technology infrastructure requirements, and limited IT staffing constrain adoption at hospitals that could benefit most from documentation time savings. Addressing equity requires subsidized access programs, shared service models, and vendor pricing that enables universal access.
Future AI documentation will evolve from passive note-taking toward active clinical partnership, proactively surfacing patient history, suggesting clinical actions, and integrating multimodal data from imaging, vitals, and wearables. Agentic documentation systems will pre-populate orders, coordinate follow-up care, and provide real-time clinical decision support embedded within the documentation workflow. The clinical note will transform from a retrospective record into a forward-looking tool that actively improves patient care.